

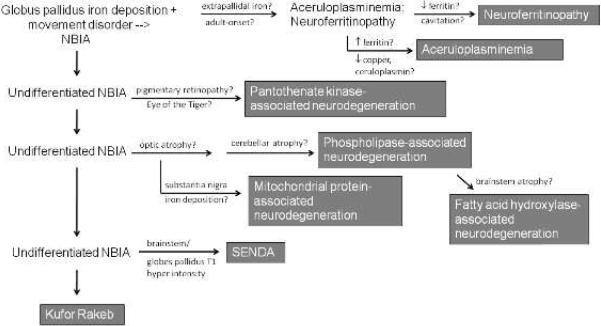
Neurodegeneration with brain iron accumulation: a diagnostic algorithm
- PMID: 22704259
- PMCID: PMC3381651
- DOI: 10.1016/j.spen.2012.04.001
Neurodegeneration with brain iron accumulation: a diagnostic algorithm
Abstract
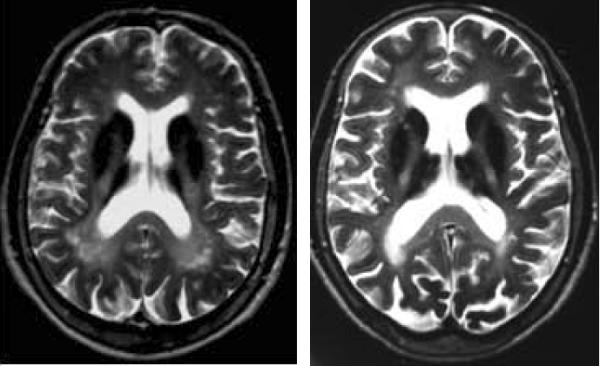
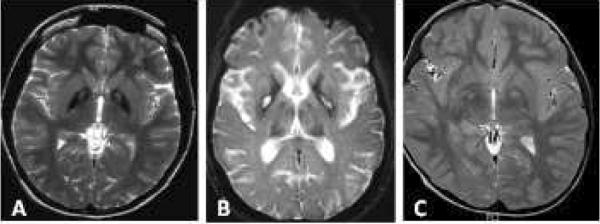
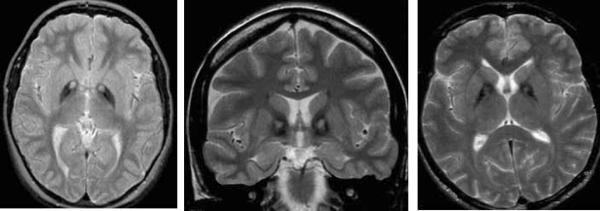
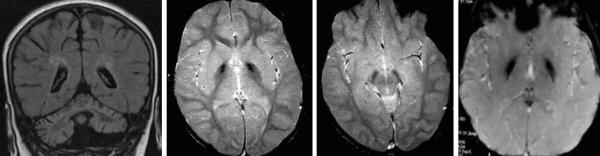
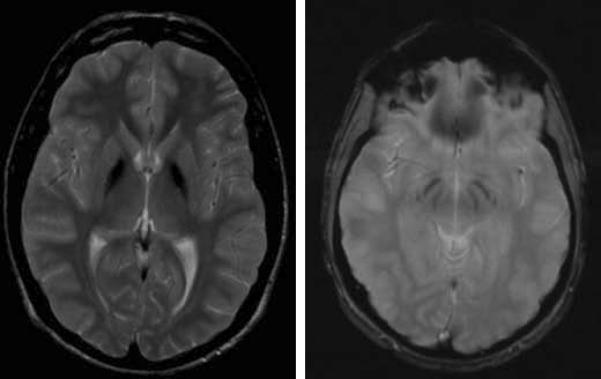
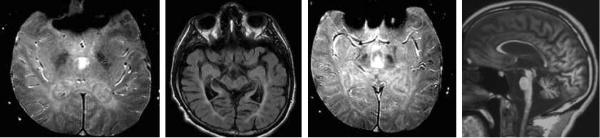
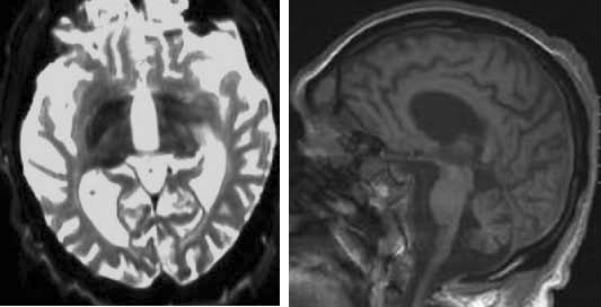
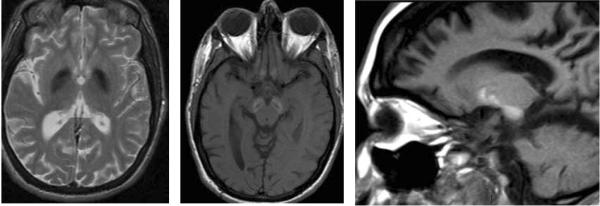
The diagnosis of neurodegeneration with brain iron accumulation (NBIA) can be challenging, particularly given recent advances in NBIA genetics and clinical nosology. Although atypical cases continue to challenge physicians, by considering clinical features along with relevant neuroimaging findings, the diagnosis of NBIA can be made confidently. In addition, the identification of genetically distinct forms of NBIA allows clinicians to better provide prognostic and family counseling services to families and may have relevance in the near future as clinical trials become available. We describe a heuristic approach to NBIA diagnosis, identify important differential considerations, and demonstrate important neuroimaging features to aid in the diagnosis.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Autti T, Joensuu R, Aberg L. Decreased T2 signal in the thalami may be a sign of lysosomal storage disease. Neuroradiology. 2007 Jul;49(7):571–8. - PubMed
-
- Bartzokis G, Cummings J, Perlman S, Hance DB, Mintz J. Increased basal ganglia iron levels in Huntington disease. Arch Neurol. 1999 May;56(5):569–74. - PubMed
-
- Chinnery PF, Crompton DE, Birchall D, Jackson MJ, Coulthard A, Lombès A, Quinn N, Wills A, Fletcher N, Mottershead JP, Cooper P, Kellett M, Bates D, Burn J. Clinical features and natural history of neuroferritinopathy caused by the FTL1 460InsA mutation. Brain. 2007 Jan;130(Pt 1):110–9. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
