

A comprehensive comparison of IMRT and VMAT plan quality for prostate cancer treatment
- PMID: 22704703
- PMCID: PMC3805837
- DOI: 10.1016/j.ijrobp.2011.09.015
A comprehensive comparison of IMRT and VMAT plan quality for prostate cancer treatment
Abstract
Purpose: We performed a comprehensive comparative study of the plan quality between volumetric-modulated arc therapy (VMAT) and intensity-modulated radiation therapy (IMRT) for the treatment of prostate cancer.
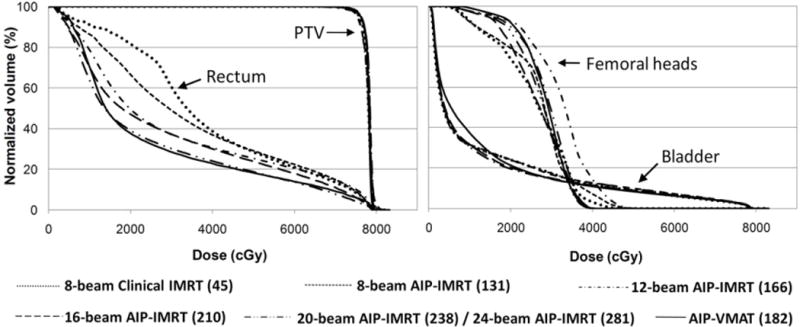
Methods and materials: Eleven patients with prostate cancer treated at our institution were randomly selected for this study. For each patient, a VMAT plan and a series of IMRT plans using an increasing number of beams (8, 12, 16, 20, and 24 beams) were examined. All plans were generated using our in-house-developed automatic inverse planning (AIP) algorithm. An existing eight-beam clinical IMRT plan, which was used to treat the patient, was used as the reference plan. For each patient, all AIP-generated plans were optimized to achieve the same level of planning target volume (PTV) coverage as the reference plan. Plan quality was evaluated by measuring mean dose to and dose-volume statistics of the organs at risk, especially the rectum, from each type of plan.
Results: For the same PTV coverage, the AIP-generated VMAT plans had significantly better plan quality in terms of rectum sparing than the eight-beam clinical and AIP-generated IMRT plans (p < 0.0001). However, the differences between the IMRT and VMAT plans in all the dosimetric indices decreased as the number of beams used in IMRT increased. IMRT plan quality was similar or superior to that of VMAT when the number of beams in IMRT was increased to a certain number, which ranged from 12 to 24 for the set of patients studied. The superior VMAT plan quality resulted in approximately 30% more monitor units than the eight-beam IMRT plans, but the delivery time was still less than 3 min.
Conclusions: Considering the superior plan quality as well as the delivery efficiency of VMAT compared with that of IMRT, VMAT may be the preferred modality for treating prostate cancer.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
CONFLICTS OF INTEREST NOTIFICATION
There are no actual or potential conflicts of interest.
Figures










References
-
- Otto K. Volumetric modulated arc therapy: IMRT in a single gantry arc. Med Phys. 2008;35:310–317. - PubMed
-
- Cozzi L, Dinshaw KA, Shrivastava SK, et al. A treatment planning study comparing volumetric arc modulation with RapidArc and fixed field IMRT for cervix uteri radiotherapy. Radiotherapy and Oncology. 2008;89:180–191. - PubMed
-
- Palma D, Vollans E, James K, et al. Volumetric Modulated Arc Therapy for Delivery of Prostate Radiotherapy: Comparison with Intensity-Modulated Radiotherapy and Three-Dimensional Conformal Radiotherapy. Int J Radiat Oncol Biol Phys. 2008;72:996–1001. - PubMed
-
- Popescu CC, Olivotto IA, Beckham WA, et al. Volumetric Modulated Arc Therapy Improves Dosimetry and Reduces Treatment Time Compared to Conventional Intensity-Modulated Radiotherapy for Locoregional Radiotherapy of Left-Sided Breast Cancer and Internal Mammary Nodes. Int J Radiat Oncol Biol Phys. 2008;76:287–295. - PubMed
-
- Bedford JL. Treatment planning for volumetric modulated arc therapy. Med Phys. 2009;36:5128–5138. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
