

Variation in outcomes for risk-stratified pediatric cardiac surgical operations: an analysis of the STS Congenital Heart Surgery Database
- PMID: 22704799
- PMCID: PMC4006082
- DOI: 10.1016/j.athoracsur.2012.01.105
Variation in outcomes for risk-stratified pediatric cardiac surgical operations: an analysis of the STS Congenital Heart Surgery Database
Abstract
Background: We evaluated outcomes for groups of risk-stratified operations in The Society of Thoracic Surgeons Congenital Heart Surgery Database to provide contemporary benchmarks and examine variation between centers.
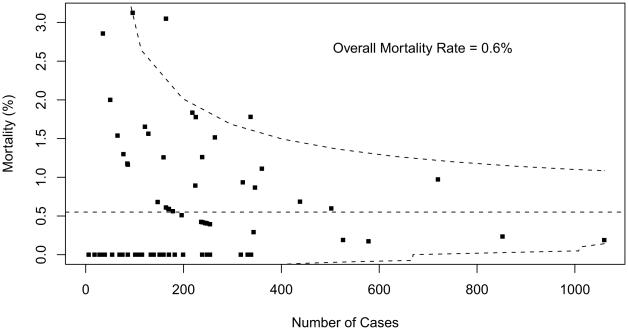
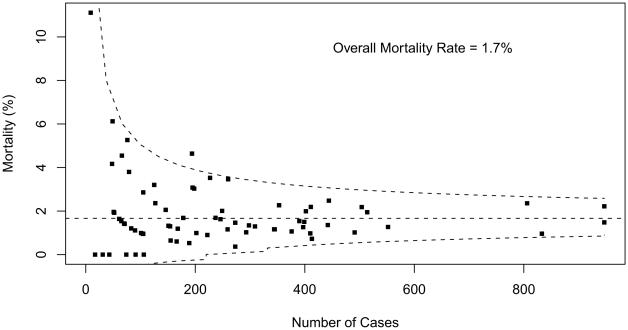
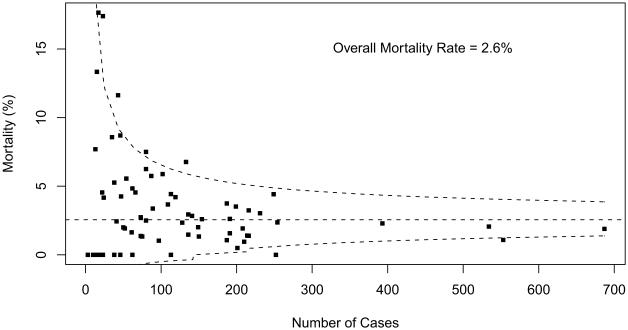
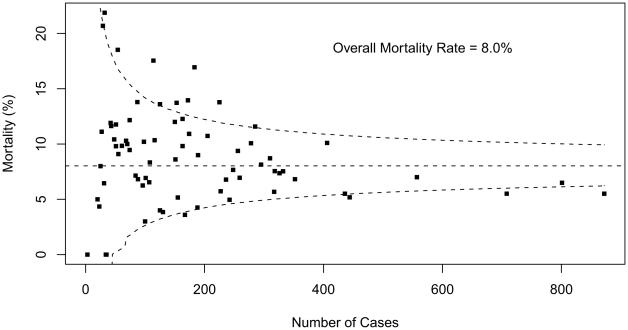
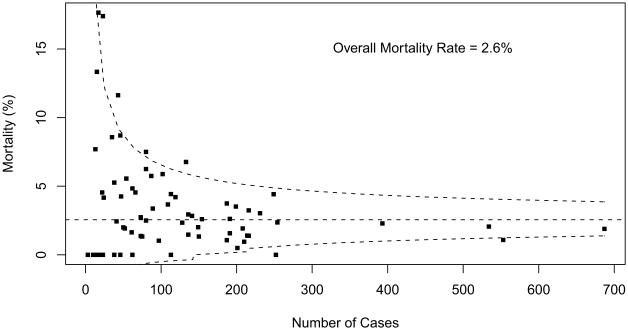
Methods: Patients undergoing surgery from 2005 to 2009 were included. Centers with more than 10% missing data were excluded. Discharge mortality and postoperative length of stay (PLOS) among patients discharged alive were calculated for groups of risk-stratified operations using the five Society of Thoracic Surgeons-European Association for Cardio-Thoracic Surgery Congenital Heart Surgery mortality categories (STAT Mortality Categories). Power for analyzing between-center differences in outcome was determined for each STAT Mortality Category. Variation was evaluated using funnel plots and Bayesian hierarchical modeling.
Results: In this analysis of risk-stratified operations, 58,506 index operations at 73 centers were included. Overall discharge mortality (interquartile range among programs with more than 10 cases) was as follows: STAT Category 1=0.55% (0% to 1.0%), STAT Category 2=1.7% (1.0% to 2.2%), STAT Category 3=2.6% (1.1% to 4.4%), STAT Category 4=8.0% (6.3% to 11.1%), and STAT Category 5=18.4% (13.9% to 27.9%). Funnel plots with 95% prediction limits revealed the number of centers characterized as outliers by STAT Mortality Categories was as follows: Category 1=3 (4.1%), Category 2=1 (1.4%), Category 3=7 (9.7%), Category 4=13 (17.8%), and Category 5=13 (18.6%). Between-center variation in PLOS was analyzed for all STAT Categories and was greatest for STAT Category 5 operations.
Conclusions: This analysis documents contemporary benchmarks for risk-stratified pediatric cardiac surgical operations grouped by STAT Mortality Categories and the range of outcomes among centers. Variation was greatest for the more complex operations. These data may aid in the design and planning of quality assessment and quality improvement initiatives.
Copyright © 2012 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Jacobs JP, Jacobs ML, Mavroudis C, Lacour-Gayet FG, Tchervenkov CI. Executive summary: The Society of Thoracic Surgeons congenital heart surgery database—twelfth harvest (January 1, 2006 -December 31, 2009) The Society of Thoracic Surgeons and Duke Clinical Research Institute, Duke University Medical Center; Durham, North Carolina: Spring 2010 Harvest.
-
- Jacobs ML, Jacobs JP, Franklin RCG, et al. Databases for assessing the outcomes of the treatment of patients with congenital and paediatric cardiac disease—the perspective of cardiac surgery. Cardiol Young. 2008;18(Suppl 2):101–15. - PubMed
-
- Jacobs JP, Maruszewski B, Kurosawa H, et al. Congenital heart surgery databases around the world: do we need a global database? Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2010;13:3–19. - PubMed
-
- Jacobs ML, Mavroudis C, Jacobs JP, et al. Report of the 2005 STS congenital heart surgery practice and manpower survey: a report from the STS Work Force on Congenital Heart Surgery. Ann Thorac Surg. 2006;82:1152–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
