

Life-saving percutaneous intervention in young patient with massive pulmonary embolism
- PMID: 22705620
- PMCID: PMC6081019
- DOI: 10.5144/0256-4947.2012.433
Life-saving percutaneous intervention in young patient with massive pulmonary embolism
Abstract
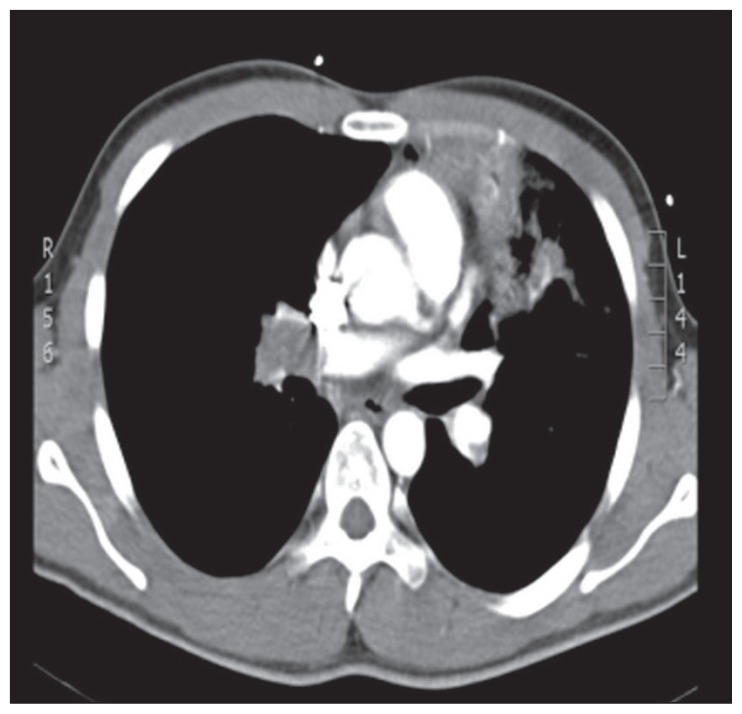
Massive pulmonary embolism (PE) is not an uncommon condition, and it usually carries a high risk of mortality. It is one of the fatal conditions that commonly affect young patients. A definitive treatment for patients with massive PE is still lacking, and surgical intervention carries a substantial mortality risk. Thus, percutaneous intervention (clot fragmentation and/or aspiration) remains an option in some patients, specifically in those with a risk of bleeding, contraindicating the use of thrombolysis. There have been no randomized trials to validate percutaneous intervention in massive PE. A sufficient level of evidence is still lacking, and its use depends upon the expert committee's opinion and study of previous case reports. We present a 23-year-old man with first onset massive PE secondary to protein C deficiency, who was treated successfully with the combination of systemic thrombolysis and percutaneous interventions.
Figures








References
-
- Eid-Lidt G, Gaspar J, Sandoval J, de los Santos FD, Pulido T, González Pacheco H, et al. Combined clot fragmentation and aspiration in patients with acute pulmonary embolism. Chest. 2008;134:54–60. - PubMed
-
- Capstick T, Henry MT. Efficacy of thrombolytic agents in the treatment of pulmonary embolism. Eur Respir J. 2005;26:864–74. - PubMed
-
- Torbicki A, Perrier A, Konstantinides S, Agnelli G, Galiè N, Pruszczyk P, et al. Guidelines on the diagnosis and management of acute pulmonary embolism. The Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC) Eur Heart J. 2008;29:2276–15. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical