

Characteristics and outcomes of methicillin-resistant staphylococcus aureus bloodstream infections in patients with cancer treated with vancomycin: 9-year experience at a comprehensive cancer center
- PMID: 22707509
- PMCID: PMC3481899
- DOI: 10.1634/theoncologist.2012-0029
Characteristics and outcomes of methicillin-resistant staphylococcus aureus bloodstream infections in patients with cancer treated with vancomycin: 9-year experience at a comprehensive cancer center
Abstract
Background: Methicillin-resistant Staphylococcus aureus (MRSA) bloodstream infections (BSIs) can cause significant morbidity and mortality in patients with cancer. However, data on outcomes of patients treated with vancomycin are lacking.
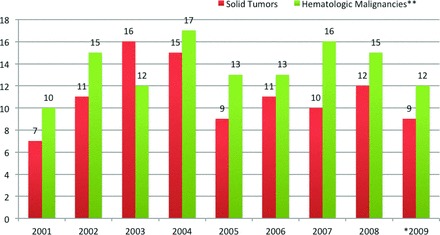
Methods: We identified 223 patients with cancer who developed MRSA BSIs between January 2001 and June 2009 and were treated with vancomycin. Treatment failure was defined as death within 60 days of infection, persistent bacteremia ≥5 days, fever ≥4 days, recurrence or relapse, and secondary MRSA infection.
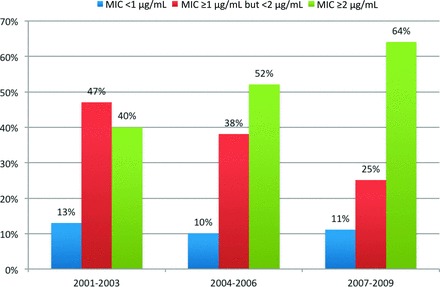
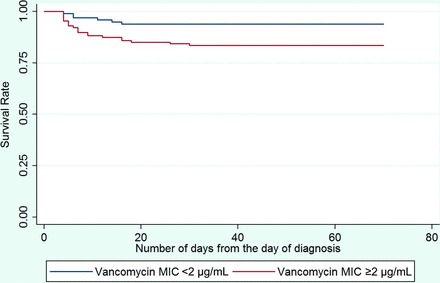
Results: The treatment failure rate was 52% (116 of 223 patients). These patients were more likely to have been hospitalized, been treated with steroids within the previous 3 months, developed acute respiratory distress syndrome, required mechanical ventilation, required intensive care unit care, and community-onset infections (all p < .05). Risk factors for MRSA-associated mortality (27 of 223 patients; 12%) included hematologic malignancy and hematopoietic stem cell transplantation, community-onset infection, secondary BSI, MRSA with minimum inhibitory concentration (MIC) ≥2.0 μg/mL, mechanical ventilation, and a late switch to an alternative therapy (≥4 days after treatment failure; all p < .05). On multivariate analysis, mechanical ventilation and recent hospitalization were identified as independent predictors of vancomycin failure, and community-onset infection, secondary BSIs, and MIC ≥2 μg/mL were identified as significant predictors of MRSA-associated mortality.
Conclusions: We found a high treatment failure rate for vancomycin in patients with cancer and MRSA BSIs, as well as a higher mortality. A vancomycin MIC ≥2 μg/mL was an independent predictor of MRSA-associated mortality. An early switch to an alternative therapy at the earliest sign of failure may improve outcome.
Conflict of interest statement
Figures
References
-
- Steinberg JP, Clark CC, Hackman BO. Nosocomial and community-acquired Staphylococcus aureus bacteremias from 1980 to 1993: Impact of intravascular devices and methicillin resistance. Clin Infect Dis. 1996;23:255–259. - PubMed
-
- Soriano A, Martinez JA, Mensa J, et al. Pathogenic significance of methicillin resistance for patients with Staphylococcus aureus bacteremia. Clin Infect Dis. 2000;30:368–373. - PubMed
-
- National Nosocomial Infections Surveillance (NNIS) report, data summary from October 1986-April 1996, issued May 1996. A report from the National Nosocomial Infections Surveillance (NNIS) system. Am J Infect Control. 1996;24:380–388. - PubMed
-
- Fowler VG, Jr., Sanders LL, Sexton DJ, et al. Outcome of Staphylococcus aureus bacteremia according to compliance with recommendations of infectious diseases specialists: Experience with 244 patients. Clin Infect Dis. 1998;27:478–486. - PubMed
-
- Mylotte JM, McDermott C, Spooner JA. Prospective study of 114 consecutive episodes of Staphylococcus aureus bacteremia. Rev Infect Dis. 1987;9:891–907. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
