

Defining neurocognitive impairment in HIV: deficit scores versus clinical ratings
- PMID: 22708483
- PMCID: PMC3848322
- DOI: 10.1080/13854046.2012.694479
Defining neurocognitive impairment in HIV: deficit scores versus clinical ratings
Abstract
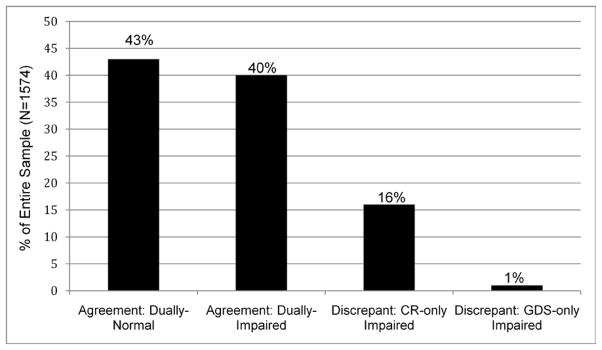
Because HIV-related neurocognitive impairment is usually mild and variable, clinical ratings (CR) and global deficit scores (GDS) are recommended for detecting HIV-associated neurocognitive disorders (HAND). The CR approach requires impairment in at least two ability domains while the GDS considers number and severity of impairments across all measures. We examined classification agreement and clinical correlates of the two methods. Neurocognitive functioning of 1574 HIV-infected participants was assessed via a comprehensive, seven-domain neuropsychological battery. Global neurocognitive impairment was defined for each participant independently by CR and GDS. Participants were classified into four categories (Dually-normal, [impaired by] CR-only, [impaired by] GDS-only, or Dually-impaired). There was 83% concordance between CR and GDS classifications; in total, 56% of participants were deemed impaired by CR and 41% were classified as impaired by GDS. Impairment by GDS virtually guaranteed CR impairment, but 16% of participants were additionally classified as impaired only by CR. As compared to Dually-normal participants, those classified as Dually and CR-only impaired were more likely to have AIDS, have more severe co-occurring conditions, have more severe depressive symptoms, be unemployed, and have more everyday functioning complaints (ps < .05). Impairment classifications of the two methods were in high agreement; however, more people were classified as impaired using the CR approach compared to the GDS approach. Those impaired according to CR-only showed fewer neurocognitive and functional deficits than the Dually-impaired participants, but more of these deficits than Dually-normal participants. The CR approach may be most appropriate for detecting more subtle forms of neurocognitive impairment. Clinicians and researchers should recognize the strengths and weaknesses of each method when evaluating neurocognitive complications in HIV.
Conflict of interest statement
Authors report no conflicts of interest affecting this article.
Figures
References
-
- Butters N, Grant I, Haxby J, Judd LL, Martin A, Stover E. Assessment of Aids-related cognitive changes: Recommendations of NIMH workshop on neuropsychological assessment approaches. Journal of Clinical and Experimental Neuropsychology. 1990;12(6):963–978. - PubMed
-
- Carey C, Woods SP, Gonzalez R, Conover E, Marcotte TD, Heaton RK. Predictive validity of Global Deficit Scores in detecting neuropsychological impairment in HIV infection. Journal of Clinical and Experimental Neuropsychology. 2004;26(3):307–319. - PubMed
-
- Center for Disease Control. 1993 revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. Morbidity and Mortality Weekly Report. 1992;41(Suppl 44-17):1–19. - PubMed
-
- Gonzalez R, Heaton RK, Moore DJ, Letendre S, Elliott R, Grant I for the HNRC Group. Computerizes reaction time battery versus a traditional neuropsychological battery: Detecting HIV-related impairments. Journal of the International Neuropsychological Society. 2003;9:64–71. - PubMed
-
- Heaton RK, Kirson D, Velin RA, Grant I. the HNRC Group. The utility of clinical ratings for detecting cognitive change in HIV infection. In: Grant I, Markin A, editors. psychology of HIV infection. New York: Oxford University Press; 1994. pp. 188–206.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials