

The pathogenesis of atrial and atrioventricular septal defects with special emphasis on the role of the dorsal mesenchymal protrusion
- PMID: 22709652
- PMCID: PMC3389176
- DOI: 10.1016/j.diff.2012.05.006
The pathogenesis of atrial and atrioventricular septal defects with special emphasis on the role of the dorsal mesenchymal protrusion
Abstract
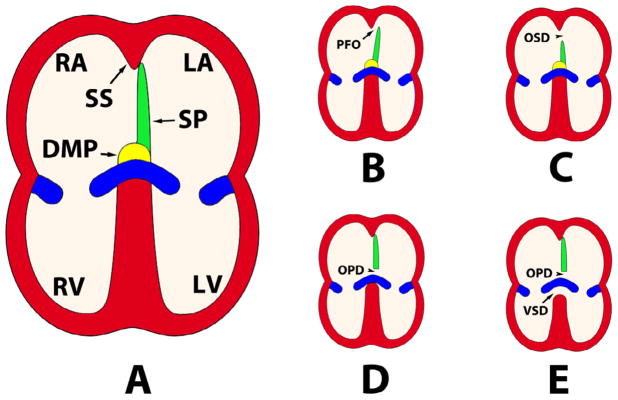
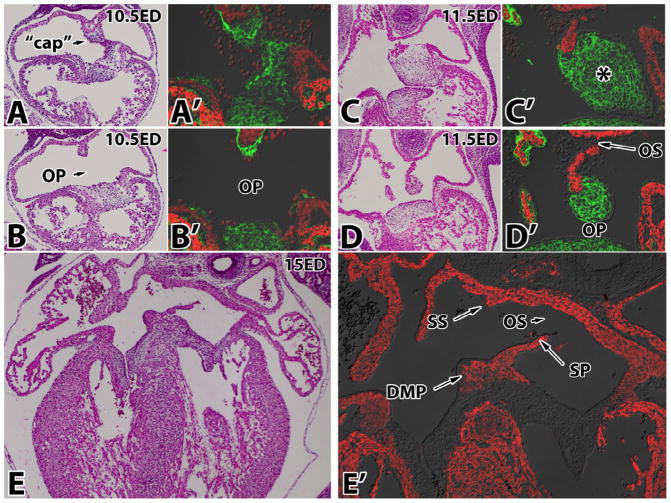
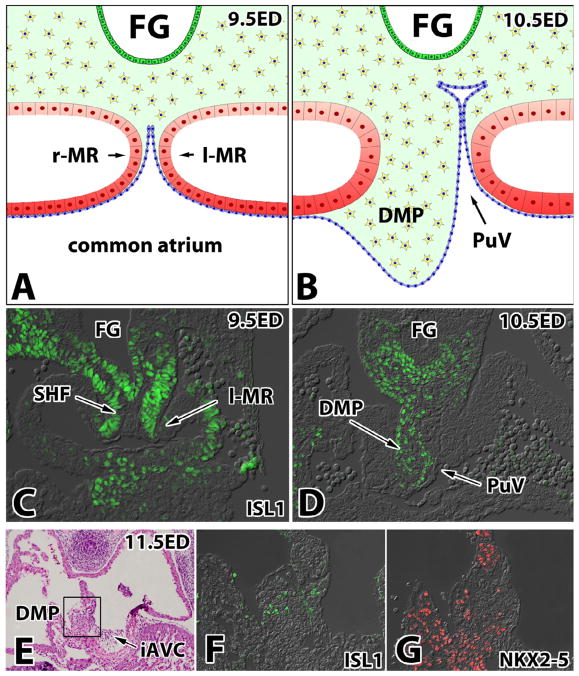
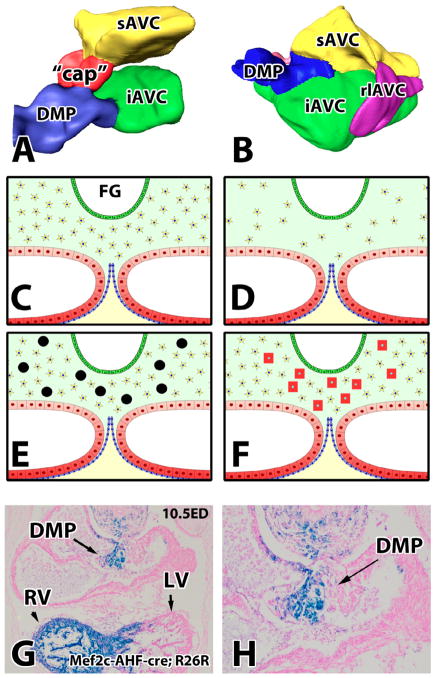
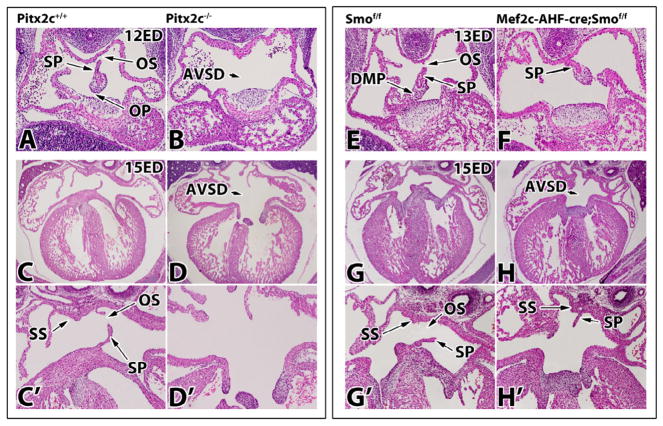
Partitioning of the four-chambered heart requires the proper formation, interaction and fusion of several mesenchymal tissues derived from different precursor populations that together form the atrioventricular mesenchymal complex. This includes the major endocardial cushions and the mesenchymal cap of the septum primum, which are of endocardial origin, and the dorsal mesenchymal protrusion (DMP), which is derived from the Second Heart Field. Failure of these structures to develop and/or fully mature results in atrial septal defects (ASDs) and atrioventricular septal defects (AVSD). AVSDs are congenital malformations in which the atria are permitted to communicate due to defective septation between the inferior margin of the septum primum and the atrial surface of the common atrioventricular valve. The clinical presentation of AVSDs is variable and depends on both the size and/or type of defect; less severe defects may be asymptomatic while the most severe defect, if untreated, results in infantile heart failure. For many years, maldevelopment of the endocardial cushions was thought to be the sole etiology of AVSDs. More recent work, however, has demonstrated that perturbation of DMP development also results in AVSD. Here, we discuss in detail the formation of the DMP, its contribution to cardiac septation and describe the morphological features as well as potential etiologies of ASDs and AVSDs.
Copyright © 2012 International Society of Differentiation. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Abu-Issa R, Kirby ML. Heart field: from mesoderm to heart tube. Annu Rev Cell Dev Biol. 2007;23:45–68. - PubMed
-
- Affolter M, Weijer CJ. Signaling to cytoskeletal dynamics during chemotaxis. Dev Cell. 2005;9:19–34. - PubMed
-
- Allen WE, Jones GE, Pollard JW, Ridley AJ. Rho, Rac and Cdc42 regulate actin organization and cell adhesion in macrophages. J Cell Sci. 1997;110 (Pt 6):707–720. - PubMed
-
- Anderson RH, Brown NA, Moorman AF. Development and structures of the venous pole of the heart. Dev Dyn. 2006;235:2–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
