

Neuronal autoantigens--pathogenesis, associated disorders and antibody testing
- PMID: 22710628
- PMCID: PMC3718498
- DOI: 10.1038/nrneurol.2012.99
Neuronal autoantigens--pathogenesis, associated disorders and antibody testing
Abstract
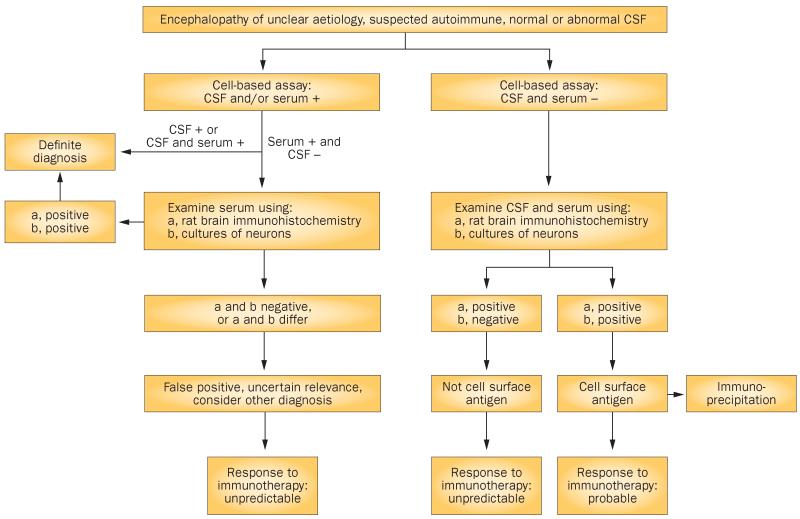
The discovery of disorders that are associated with antibodies to neuronal cell-surface proteins has led to a paradigm shift in our understanding of CNS autoimmunity. These disorders can occur in patients with or without cancer-often children or young adults who develop psychosis, catatonic or autistic features, memory problems, abnormal movements, or seizures that were previously considered idiopathic. The autoantigens in such cases have crucial roles in synaptic transmission, plasticity and peripheral nerve excitability. Patients can be comatose or encephalopathic for months and yet fully recover with supportive care and immunotherapy. By contrast, disorders in which the antibodies target intracellular antigens, and in which T-cell-mediated irreversible neuronal degeneration occurs, show a considerably poorer response to treatment. In this article, we review the various targets of neuronal antibodies, focusing predominantly on autoantigens located on the cell surface or synapses-namely, N-methyl-D-aspartate receptors, α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptors, γ-aminobutyric acid receptors, leucine-rich glioma-inactivated protein 1, contactin-associated protein-like 2, and metabotropic glutamate receptors. We also provide an algorithm to identify and assess antibodies that bind to cell-surface and synaptic antigens.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
