

Projecting the benefits of antiretroviral therapy for HIV prevention: the impact of population mobility and linkage to care
- PMID: 22711905
- PMCID: PMC3491737
- DOI: 10.1093/infdis/jis401
Projecting the benefits of antiretroviral therapy for HIV prevention: the impact of population mobility and linkage to care
Abstract
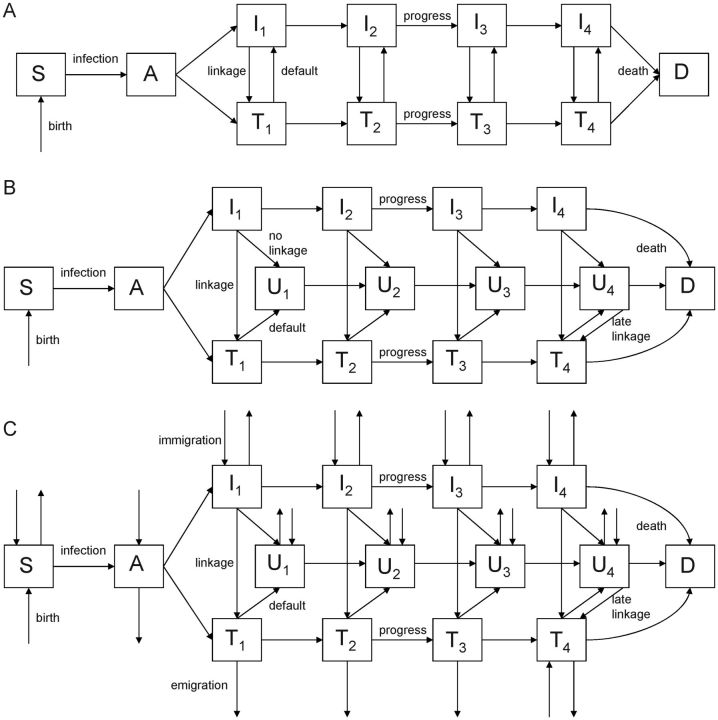
Background: Recent mathematical models suggested that frequent human immunodeficiency virus (HIV) testing with immediate initiation of antiretroviral therapy (ART) to individuals with a positive test result could profoundly curb transmission. The debate about ART as prevention has focused largely on parameter values. We aimed to evaluate structural assumptions regarding linkage to care and population mobility, which have received less attention.
Methods: We modified the linkage structure of published models of ART as prevention, such that individuals who decline initial testing or treatment do not link to care until late-stage HIV infection. We then added population mobility to the models. We populated the models with demographic, clinical, immigration, emigration, and linkage data from a South African township.
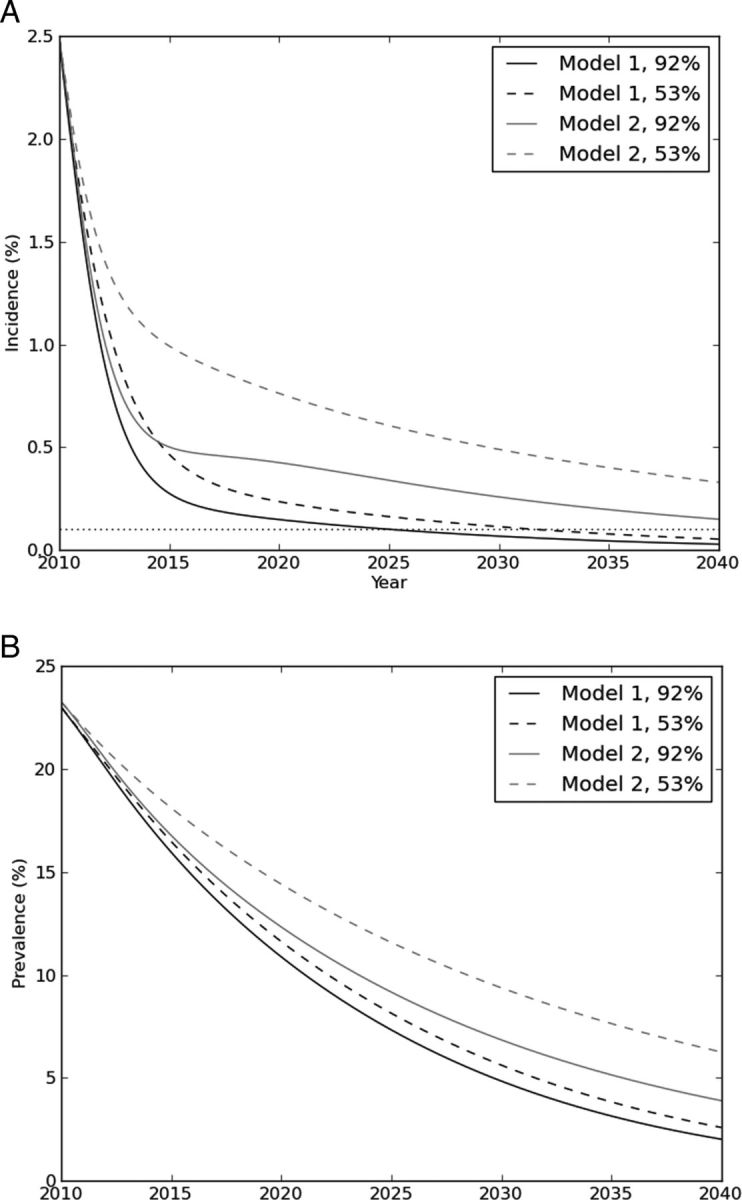
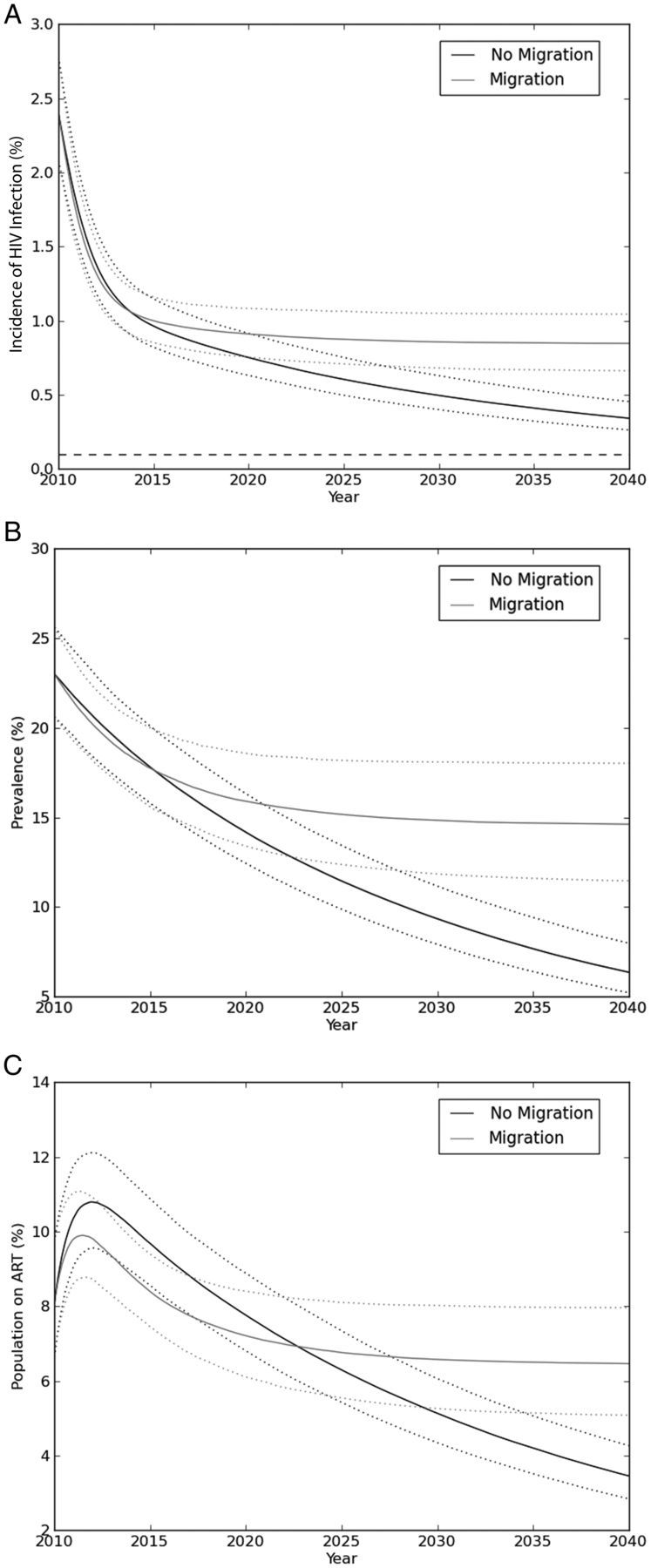
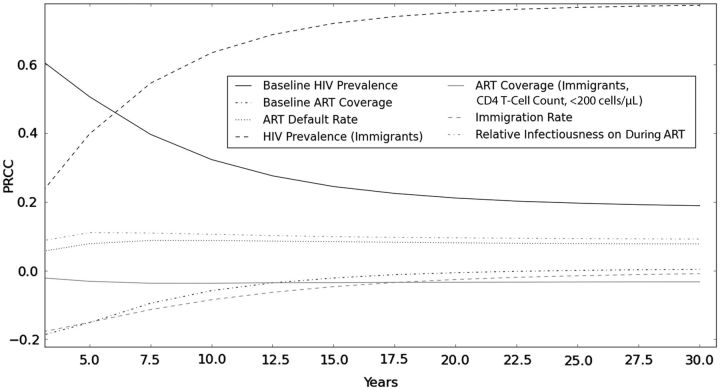
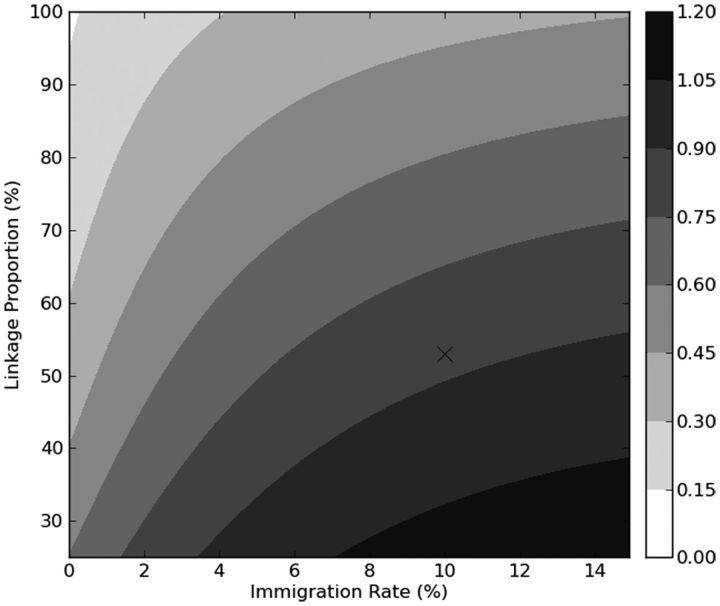
Results: In the refined linkage model, elimination of HIV transmission (defined as an incidence of <0.1%) did not occur by 30 years, even with optimistic assumptions about the linkage rate. Across a wide range of estimates, models were more sensitive to structural assumptions about linkage than to parameter values. Incorporating population mobility further attenuated the reduction in incidence conferred by ART as prevention.
Conclusions: Linkage to care and population mobility are critical features of ART-as-prevention models. Clinical trials should incorporate relevant data on linkage to care and migration to evaluate the impact of this strategy.
Figures
References
-
- Montaner JSG, Hogg R, Wood E, et al. The case for expanding access to highly active antiretroviral therapy to curb the growth of the HIV epidemic. Lancet. 2006;368:531–6. - PubMed
-
- Blower SM, Gershengorn HB, Grant RM. A tale of two futures: HIV and antiretroviral therapy in San Francisco. Science. 2000;287:650–4. - PubMed
-
- Velasco M, Castilla V, Sanz J, et al. Effect of simultaneous use of highly active antiretroviral therapy on survival of HIV patients with tuberculosis. J Acquir Immune Defic Syndr. 2009;50:148–52. - PubMed
-
- Granich RM, Gilks CF, Dye C, De Cock KM, Williams BG. Universal voluntary HIV testing with immediate antiretroviral therapy as a strategy for elimination of HIV transmission: a mathematical model. Lancet. 2009;373:48–57. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
