

Systematic Review and Meta-analysis of Pharmacological Interventions for Weight Gain from Antipsychotics and Mood Stabilizers
- PMID: 22712004
- PMCID: PMC3375952
- DOI: 10.2174/157340012798994867
Systematic Review and Meta-analysis of Pharmacological Interventions for Weight Gain from Antipsychotics and Mood Stabilizers
Abstract
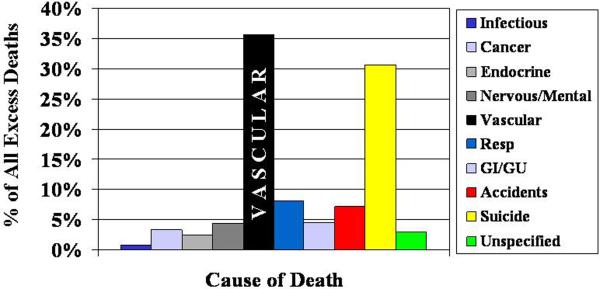
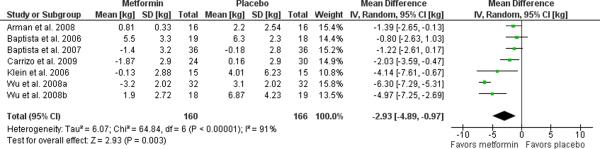
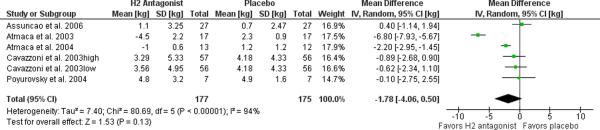
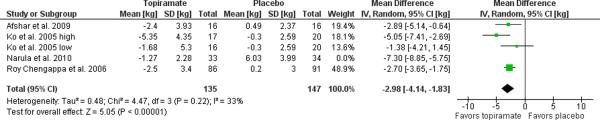
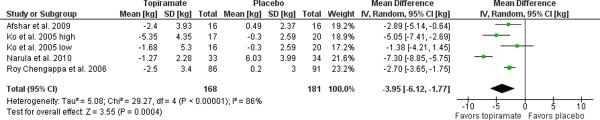
Pharmacological treatments for serious mental illness (SMI) can cause weight gain and adverse metabolic effects. Many second generation antipsychotics and mood stabilizers appear to be particularly problematic in this regard. Several studies have investigated interventions for antipsychotic-induced, or less commonly mood stabilizer -induced, weight gain. Both lifestyle and pharmacological interventions have demonstrated effectiveness. We systematically review randomized controlled trials of pharmacological interventions for weight gain related to these medications. We conducted a meta-analysis of clinical trials for the most studied agents to estimate mean weight loss: metformin (2.93 kg, 95% C.I. 0.97-4.89, p=0.003), H(2) antagonists (1.78 kg (95% C.I. -0.50-4.06, p=0.13), topiramate (3.95 kg 95% C.I. 1.77-6.12, p=0.0004), and norepinephrine reuptake inhibitors (1.30 kg (95% C.I. -0.06-2.66, p=0.06). Among the studied options for antipsychotic-related weight gain, metformin has the strongest evidence base and may improve vascular risk factors beyond obesity. The use of topiramate is also supported by the literature and may improve psychotic symptoms in those refractory to treatment. A marginal benefit is seen with norepinephrine reuptake inhibitors, and any vascular benefits from such weight loss may be counteracted by increases in blood pressure or heart rate. Pharmacological therapies may offer benefits as a means of supplementing the effects of lifestyle changes for weight loss. However, the existing evidence provides little evidence of specificity for pharmacological therapies to antipsychotic-induced weight gain and has not studied any connection between benefits and reduced incidence of diabetes mellitus or any vascular outcomes.
Figures

References
-
- Saha S, Chant D, McGrath J. A systematic review of mortality in schizophrenia: is the differential mortality gap worsening over time? Arch Gen Psychiatry. 2007;64(10):1123–31. - PubMed
-
- Murray DP, Weiner M, Prabhakar M, Fiedorowicz JG. Mania and mortality: why the excess cardiovascular risk in bipolar disorder? Curr Psychiatry Rep. 2009;11(6):475–80. - PubMed
-
- Osby U, Brandt L, Correia N, Ekbom A, Sparen P. Excess mortality in bipolar and unipolar disorder in Sweden. Arch Gen Psychiatry. 2001;58(9):844–50. - PubMed
-
- Meetoo D. Chronic diseases: the silent global epidemic. Br J Nurs. 2008;17(21):1320–5. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources