

The economic burden of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)
- PMID: 22712729
- PMCID: PMC3463640
- DOI: 10.1111/j.1469-0691.2012.03914.x
The economic burden of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)
Abstract
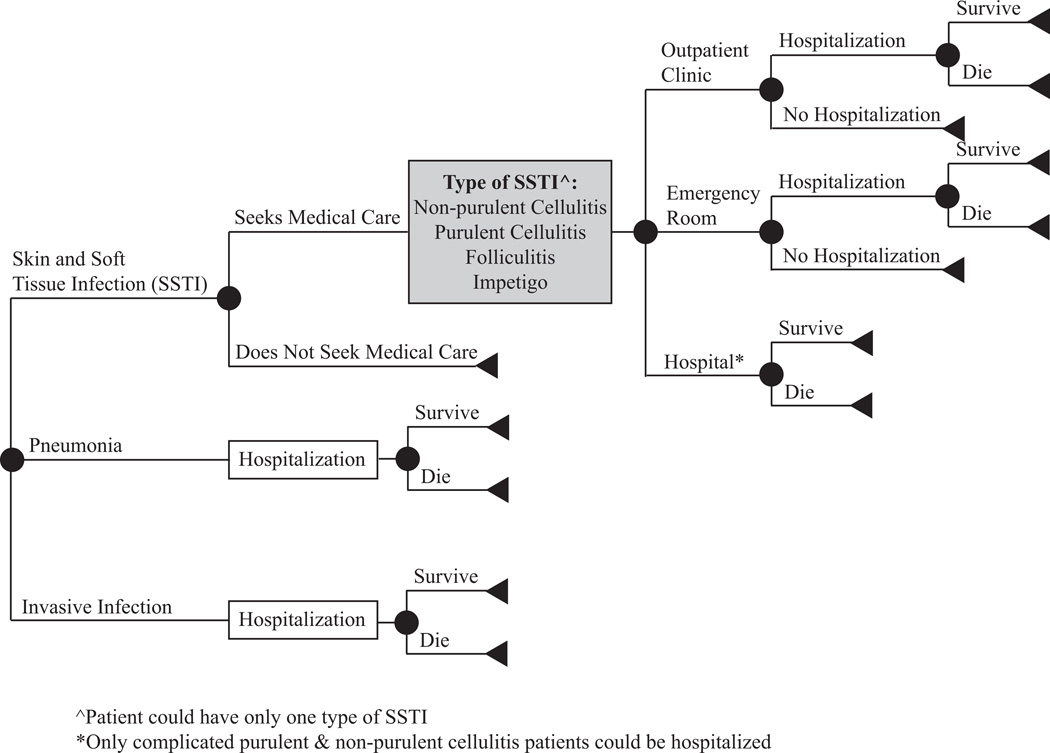
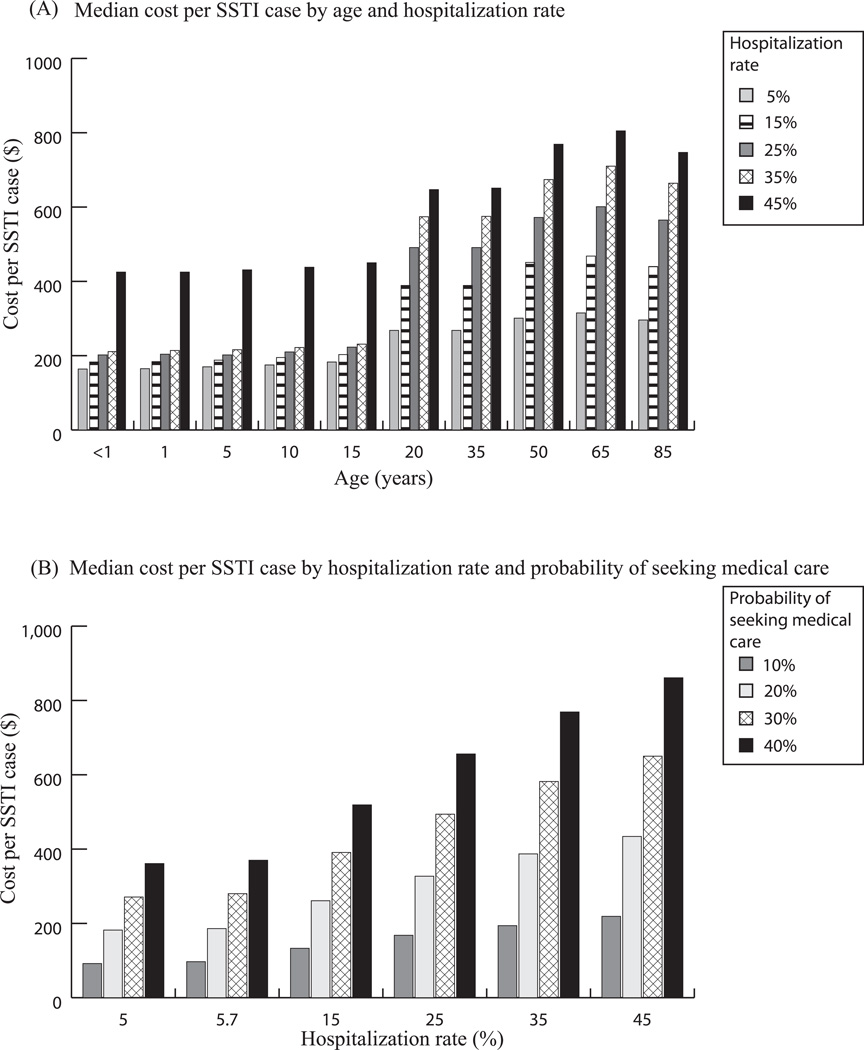
The economic impact of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) remains unclear. We developed an economic simulation model to quantify the costs associated with CA-MRSA infection from the societal and third-party payer perspectives. A single CA-MRSA case costs third-party payers $2277-$3200 and society $7070-$20 489, depending on patient age. In the United States (US), CA-MRSA imposes an annual burden of $478 million to 2.2 billion on third-party payers and $1.4-13.8 billion on society, depending on the CA-MRSA definitions and incidences. The US jail system and Army may be experiencing annual total costs of $7-11 million ($6-10 million direct medical costs) and $15-36 million ($14-32 million direct costs), respectively. Hospitalization rates and mortality are important cost drivers. CA-MRSA confers a substantial economic burden on third-party payers and society, with CA-MRSA-attributable productivity losses being major contributors to the total societal economic burden. Although decreasing transmission and infection incidence would decrease costs, even if transmission were to continue at present levels, early identification and appropriate treatment of CA-MRSA infections before they progress could save considerable costs.
© 2012 The Authors. Clinical Microbiology and Infection © 2012 European Society of Clinical Microbiology and Infectious Diseases.
Conflict of interest statement
We are not aware of any significant conflicts of interest.
Figures
References
-
- Herold BC, Immergluck LC, Maranan MC, Lauderdale DS, Gaskin RE, Boyle-Vavra S, et al. Community-acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA. 1998 Feb 25;279(8):593–598. - PubMed
-
- Otto M. Community-associated MRSA: a dangerous epidemic. Future Medicine Ltd. 2007;2(5):457–479. - PubMed
-
- Moran GJ, Krishnadasan A, Gorwitz RJ, Fosheim GE, McDougal LK, Carey RB, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006 Aug 17;355(7):666–674. - PubMed
-
- Walraven CJ, Lingenfelter E, Rollo J, Madsen T, Alexander DP. Diagnostic and Therapeutic Evaluation of Community-acquired Methicillin-resistant Staphylococcus Aureus (MRSA) Skin and Soft Tissue Infections in the Emergency Department. J Emerg Med. 2011 Apr 25; - PubMed
-
- Kluytmans-Vandenbergh MF, Kluytmans JA. Community-acquired methicillin-resistant Staphylococcus aureus: current perspectives. Clin Microbiol Infect. 2006 Mar;12(Suppl 1):9–15. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
