

Polyclonal non multiresistant methicillin resistant Staphylococcus aureus isolates from clinical cases of infection occurring in Palermo, Italy, during a one-year surveillance period
- PMID: 22713430
- PMCID: PMC3473248
- DOI: 10.1186/1476-0711-11-17
Polyclonal non multiresistant methicillin resistant Staphylococcus aureus isolates from clinical cases of infection occurring in Palermo, Italy, during a one-year surveillance period
Abstract
Background: The evolving epidemiology of methicillin resistant Staphylococcus aureus (MRSA) is characterized by the emergence of infections caused by non multiresistant MRSA carrying staphylococcal chromosomal cassette (SCC)mec IV or V in the healthcare settings. A molecular epidemiological analysis of non multiresistant MRSA isolates from four acute general hospitals was performed in Palermo, Italy, during a one year period.
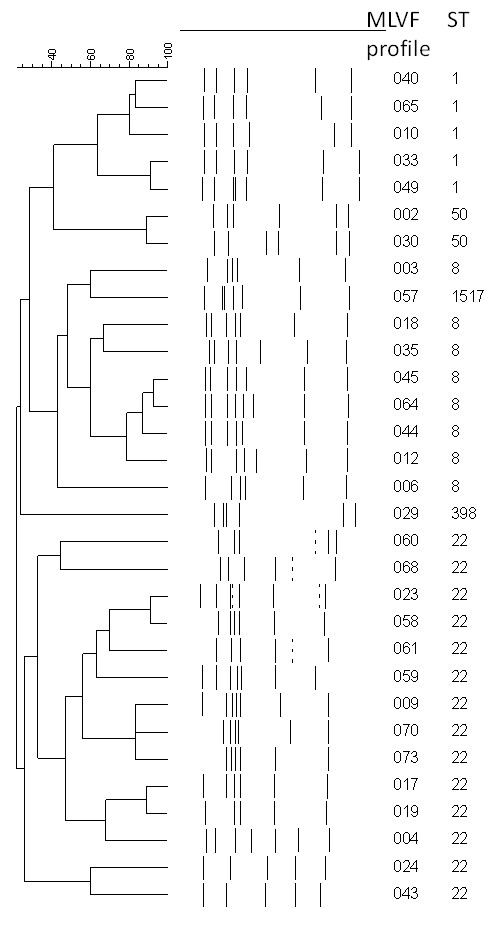
Methods: For the purpose of the study, MRSA isolates were defined as non multiresistant when they were susceptible to at least three classes of non β-lactam antibiotics. Seventy-five isolates were submitted to antimicrobial susceptibility testing, multilocus sequence typing (MLST) and polymerase chain reaction (PCR) for SCCmec, accessory gene regulator (agr) groups, arginine catabolic mobile element (ACME) and Panton Valentine leukocidin (PVL) toxin genes. For epidemiological typing, Multiple-Locus Variable-Number Tandem Repeat Fingerprinting (MLVF) was performed on all isolates and pulsed field gel electrophoresis (PFGE) on ST8 isolates.
Results: Non multiresistant MRSA isolates were isolated from all hospitals. Resistances to ciprofloxacin, macrolides and tetracycline were the most prevalent. MLST attributed 46 isolates with ST22, 13 with ST8, eight with ST1, three with ST50 and three with ST398. SCCmec type IV was found in all isolates. PVL was detected in one ST22 isolate. All isolates tested negative for the ACME element. MLVF identified 31 different patterns, some subtype clusters ranging in size between two and 22 isolates. The closely related PFGE patterns of the ST8 isolates differed from USA300.
Conclusions: A polyclonal circulation of non multiresistant MRSA along with blurring of boundaries between healthcare associated (HA)-MRSA and community associated (CA)-MRSA appear to be occurring in our epidemiological setting. A better understanding of spread of MRSA with the support of molecular typing can provide invaluable information in the epidemiological, microbiological and clinical fields.
Figures
References
-
- Johnson AP. Methicillin-resistantStaphylococcus aureus: the European landscape. J Antimicrob Chemother. 2011;66(Suppl 4):iv43–iv48. - PubMed
-
- Kennedy AD, Otto M, Braughton KR, Whitney AR, Chen L, Mathema B, Mediavilla JR, Byrne KA, Parkins LD, Tenover FC, Kreiswirth BN, Musser JM, De Leo FR. Epidemic community-associated methicillin-resistantStaphylococcus aureus: recent clonal expansion and diversification. Proc Natl Acad Sci Unit States Am. 2008;105:1327–1332. doi: 10.1073/pnas.0710217105. - DOI - PMC - PubMed
-
- Lesosky M, McGeer A, Simor A, Green K, Low DE, Raboud J. Effect of patterns of transferring patients among healthcare institutions on rates of nosocomial methicillin-resistantStaphylococcus aureustransmission: a Monte Carlo simulation. Infect Contr Hosp Epidemiol. 2011;32:136–147. doi: 10.1086/657945. - DOI - PubMed
-
- Naimi TS, LeDell KH, Como-Sabetti K, Borchardt SM, Boxrud DJ, Etienne J, Johnson SK, Vadenesch F, Fridkin S, O'Boyle C, Danila RN, Lynfield R. Comparison of community- and health care-associated methicillin-resistantStaphylococcus aureusinfection. JAMA. 2003;290:2976–2984. doi: 10.1001/jama.290.22.2976. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
