

Aversive and reinforcing opioid effects: a pharmacogenomic twin study
- PMID: 22713632
- PMCID: PMC3428265
- DOI: 10.1097/ALN.0b013e31825a2a4e
Aversive and reinforcing opioid effects: a pharmacogenomic twin study
Abstract
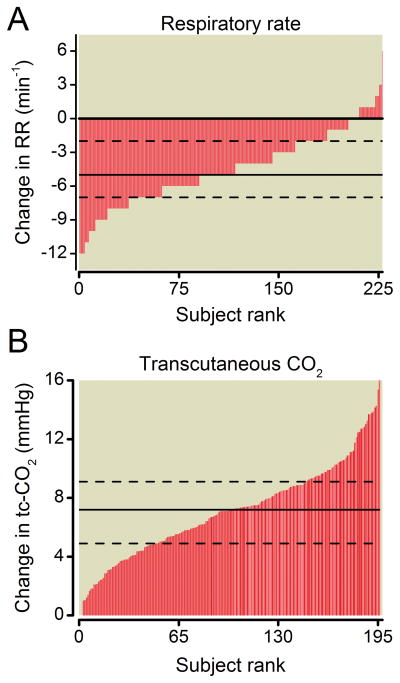
Background: The clinical utility of opioids is limited by adverse drug effects including respiratory depression, sedation, nausea, and pruritus. In addition, abuse of prescription opioids is problematic. Gaining a better understanding of the genetic and environmental mechanisms contributing to an individual's susceptibility to adverse opioid effects is essential to identify patients at risk.
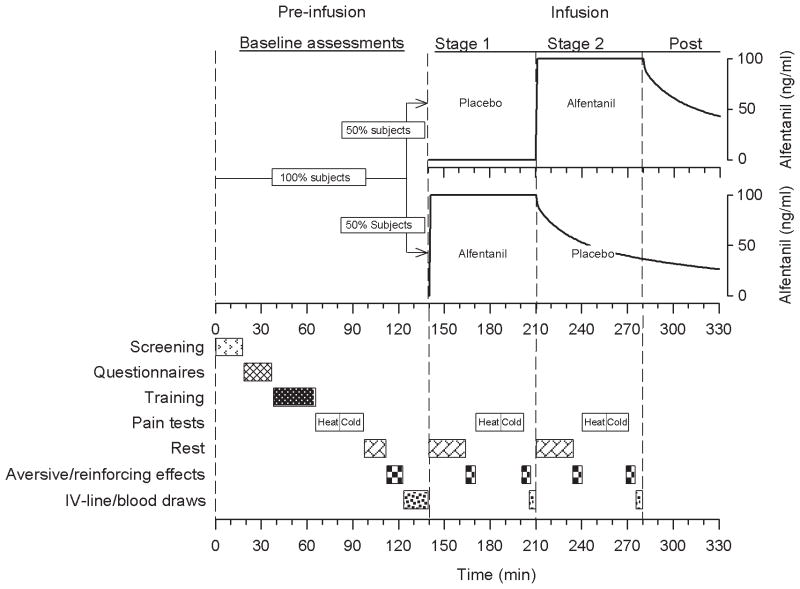
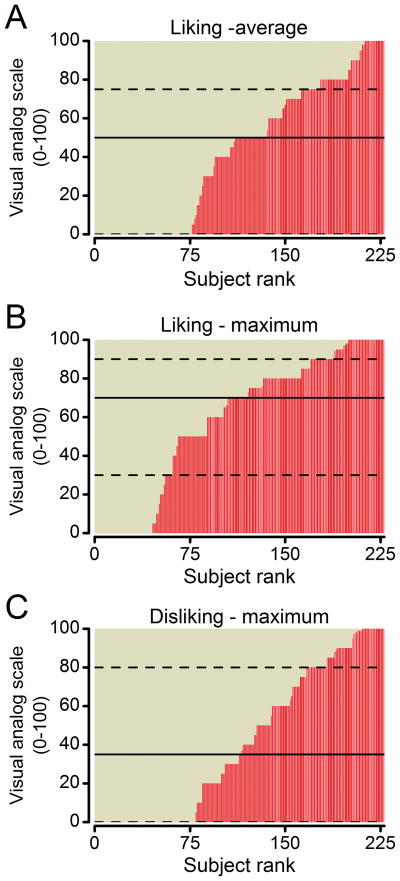
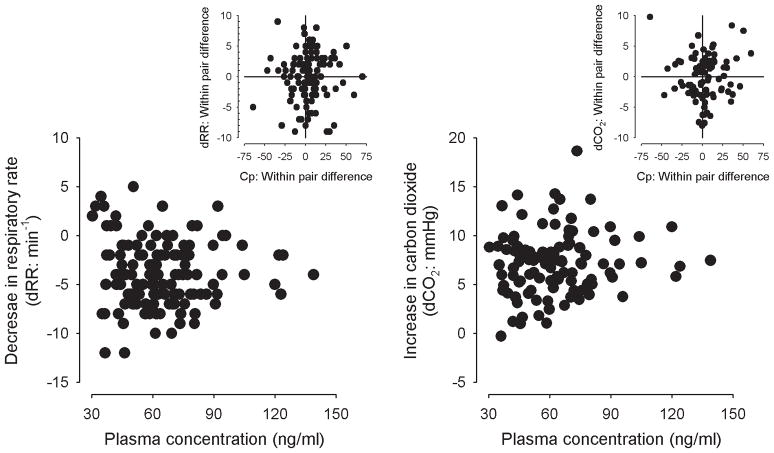
Methods: A classic twin study paradigm provided estimates for the genetic and familial (genetic and/or shared environment) contribution to acute adverse and affective opioid responses, all secondary outcomes of a larger dataset. One hundred twenty-one twin pairs were recruited in a single occasion, randomized, double-blind, and placebo-controlled study. The μ-opioid receptor agonist alfentanil and saline placebo were administered as target-controlled infusions under carefully monitored laboratory conditions. Measured outcomes included respiratory depression, sedation, nausea, pruritus, drug liking, and drug disliking. Demographic information was collected, and aspects of mood and sleep were evaluated.
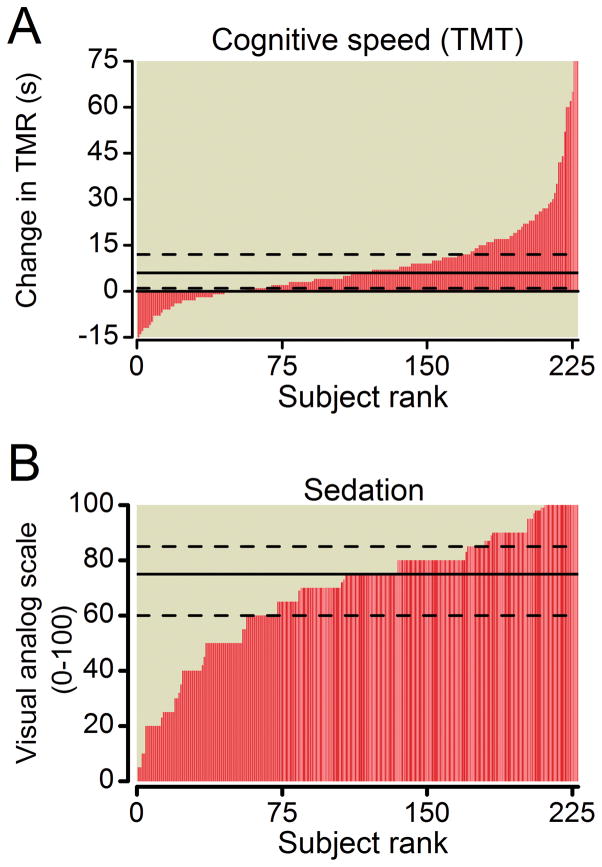
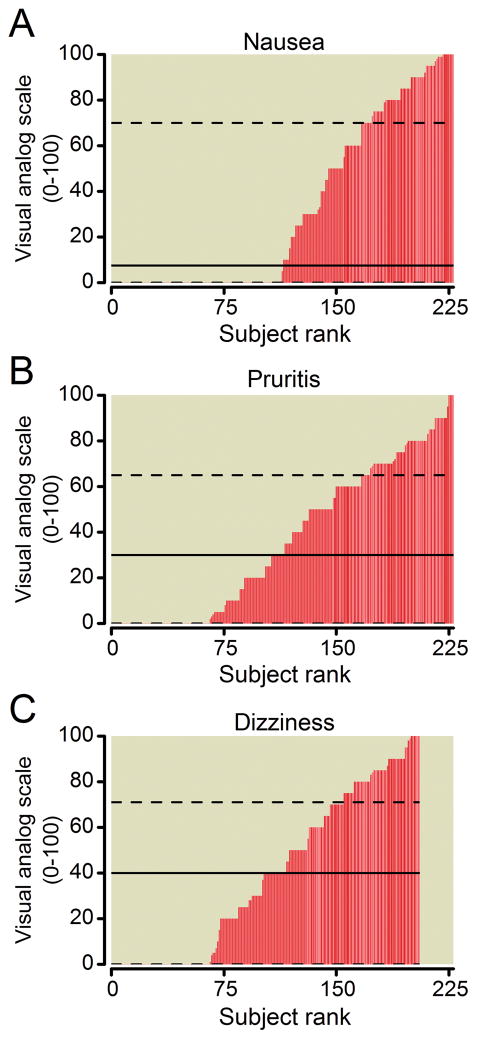
Results: Significant heritability was detected for respiratory depression (30%), nausea (59%), and drug disliking (36%). Significant familial effects were detected for sedation (29%), pruritus (38%), dizziness (32%), and drug liking (26%). Significant covariates included age, sex, race, ethnicity, education, mood, and depression. Covariates affected sedation, pruritus, drug liking and disliking, and dizziness.
Conclusions: This study demonstrates that large-scale efforts to collect quantitative and well-defined opioid response data are not only feasible but also produce data that are suitable for genetic analysis. Genetic, environmental, and demographic factors work together to control adverse and reinforcing opioid responses, but contribute differently to specific responses.
Conflict of interest statement
The authors do not have any conflict of interest.
Figures
Comment in
-
Genetic contributions to opioid side effects: helix me, helix me not.Anesthesiology. 2012 Jul;117(1):6-7. doi: 10.1097/ALN.0b013e31825a2e3f. Anesthesiology. 2012. PMID: 22713631 No abstract available.
-
Monozygotic twins: identical in name only.Anesthesiology. 2013 Jan;118(1):230. doi: 10.1097/ALN.0b013e318278c785. Anesthesiology. 2013. PMID: 23249942 No abstract available.
-
In reply.Anesthesiology. 2013 Jan;118(1):230-1. doi: 10.1097/ALN.0b013e318278e4e4. Anesthesiology. 2013. PMID: 23249943 No abstract available.
References
-
- Angst MS, Chu LF, Tingle MS, Shafer SL, Clark JD, Drover DR. No evidence for the development of acute tolerance to analgesic, respiratory depressant and sedative opioid effects in humans. Pain. 2009;142:17–26. - PubMed
-
- Dolin SJ, Cashman JN. Tolerability of acute postoperative pain managemen: Nausea, vomiting, sedation, pruritus, and urinary retention. Evidence from published data. Br J Anaesth. 2005;95:584–91. - PubMed
-
- Cashman JN, Dolin SJ. Respiratory and haemodynamic effects of acute postoperative pain management: evidence from published data. Br J Anaesth. 2004;93:212–23. - PubMed
-
- Dahan A, Aarts L, Smith TW. Incidence, Reversal, and Prevention of Opioid-induced Respiratory Depression. Anesthesiology. 2010;112:226–38. - PubMed
-
- Hagle ME, Lehr VT, Brubakken K, Shippee A. Respiratory depression in adult patients with intravenous patient-controlled analgesia. Orthop Nurs. 2004;23:18–27. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
