

A review of risk factors and timing for postoperative hematoma after thyroidectomy: is outpatient thyroidectomy really safe?
- PMID: 22714575
- PMCID: PMC3465547
- DOI: 10.1007/s00268-012-1682-1
A review of risk factors and timing for postoperative hematoma after thyroidectomy: is outpatient thyroidectomy really safe?
Abstract
Background: Although postoperative hematoma after thyroidectomy is uncommon, patients traditionally have been advised to stay overnight in the hospital for monitoring. With the growing demand for outpatient thyroidectomy, we assessed its safety and feasibility by evaluating the potential risk factors and timing of postoperative hematoma after thyroidectomy.
Methods: From 1995-2011, 3,086 consecutive patients underwent thyroidectomy at our institution; of these, 22 (0.7 %) developed a postoperative hematoma that required surgical reexploration (group I). Potential risk factors were compared between group I and those without hematoma (n = 3,045) or with hematoma but not requiring reexploration (n = 19; group II). Variables that were significant in the univariate analysis were entered into multivariate analysis by binary logistic regression analysis.
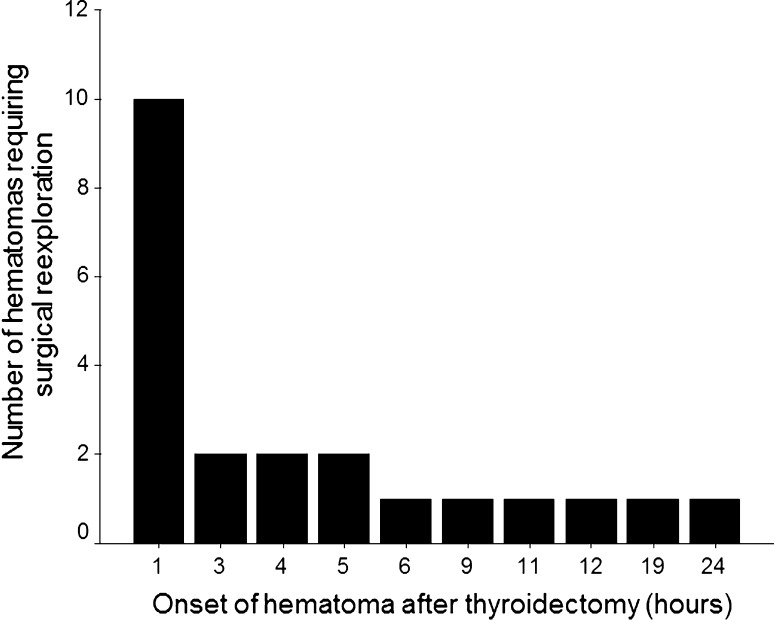
Results: Group I was significantly more likely to have undergone previous thyroid operation than group II (27.3 vs. 8.2 %, p = 0.007). The median weight of excised thyroid gland (71.8 vs. 40 g, p = 0.018) and the median size of the dominant nodule (4.1 vs. 3 cm, p = 0.004) were significantly greater in group I than group II. Previous thyroid operation (odds ratio (OR) = 4.084; 95 % confidence interval (CI), 1.105-15.098; p = 0.035) and size of dominant nodule (OR = 1.315; 95 % CI, 1.024-1.687; p = 0.032) were independent factors for hematoma. Sixteen (72.7 %) had hematoma within 6 h, whereas the other 6 (27.3 %) had hematoma at 6-24 h.
Conclusions: Previous thyroid operation and large dominant nodule were independent risk factors for hematoma requiring surgical reexploration. Given that a quarter of hematoma occurred between 6 to 24 h after surgery, routine outpatient thyroidectomy could not be recommended.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
