

Polyvascular disease and long-term cardiovascular outcomes in older patients with non-ST-segment-elevation myocardial infarction
- PMID: 22715460
- PMCID: PMC3707283
- DOI: 10.1161/CIRCOUTCOMES.111.964379
Polyvascular disease and long-term cardiovascular outcomes in older patients with non-ST-segment-elevation myocardial infarction
Abstract
Background: The impact of polyvascular disease (peripheral arterial disease [PAD] and cerebrovascular disease [CVD]) on long-term cardiovascular outcomes among older patients with acute myocardial infarction has not been well studied.
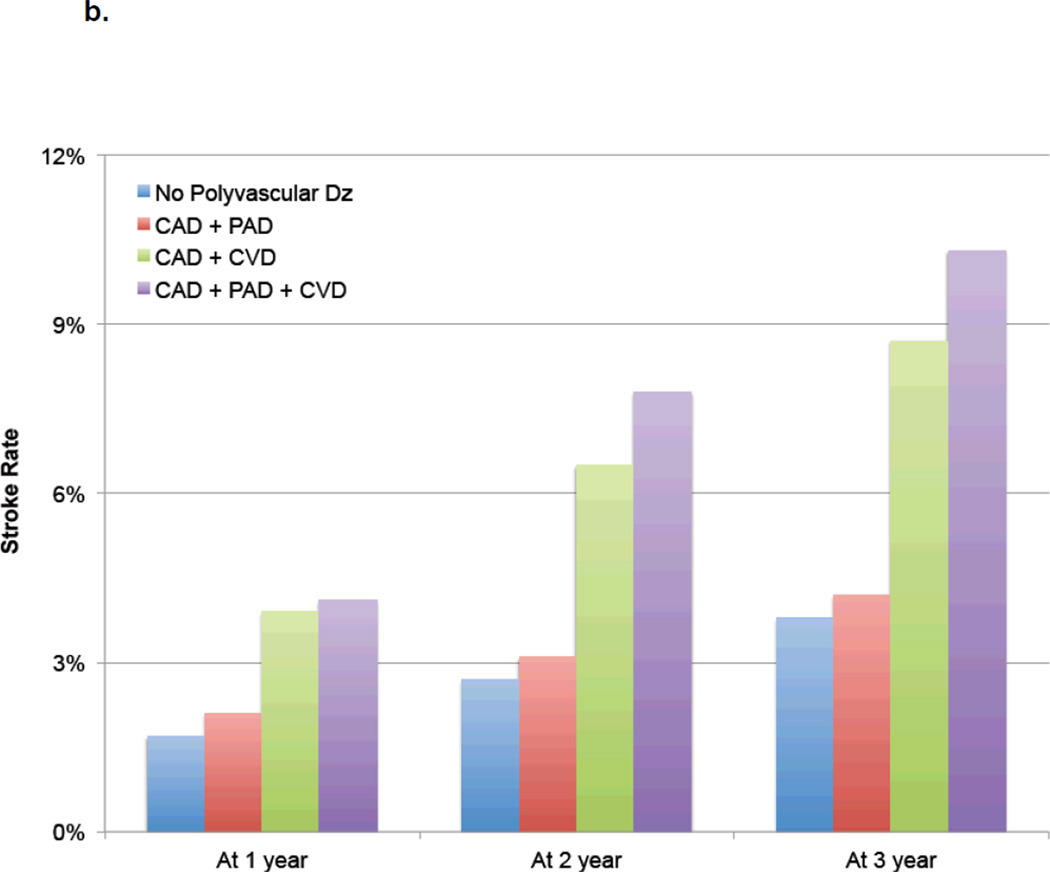
Methods and results: Patients with non-ST-segment-elevation myocardial infarction aged ≥65 years from the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines) registry who survived to hospital discharge were linked to longitudinal data from the Centers for Medicare & Medicaid Services (n=34 205). All patients were presumed to have coronary artery disease (CAD) and were classified into the following 4 groups: 10.7% with prior CVD (CAD+CVD group); 11.5% with prior PAD (CAD+PAD); 3.1% with prior PAD and CVD (CAD+PAD+CVD); and 74.7% with no polyvascular disease (CAD alone). Cox proportional hazards modeling was used to examine the hazard of long-term mortality and composite of death or readmission for myocardial infarction or stroke (median follow-up, 35 months; interquartile range, 17-49 months). Compared with the CAD alone group, patients with polyvascular disease had greater comorbidities, were less likely to undergo revascularization, and received less often recommended discharge interventions. Three-year mortality rates increased with number of arterial bed involvement as follows: 33% for CAD alone, 49% for CAD+PAD, 52% for CAD+CVD, and 59% for CAD+PAD+CVD. Relative to the CAD alone group, patients with all 3 arterial beds involved had the highest risk of long-term mortality (adjusted hazard ratio [95% CI], 1.49 [1.38-1.61]; CAD+CVD, 1.38 [1.31-1.44]; CAD+PAD, 1.29 [1.23-1.35]). Similarly, the risk of long-term composite ischemic events was highest among patients in the CAD+PAD+CVD group.
Conclusions: Among older patients with non-ST-segment-elevation myocardial infarction, those with polyvascular disease have substantially higher long-term risk for recurrent events or death. Future studies targeting greater adherence to secondary prevention strategies and novel therapies are needed to help to reduce long-term cardiovascular events in this vulnerable population.
Conflict of interest statement
Figures





References
-
- Criqui MH. Peripheral arterial disease—epidemiological aspects. Vasc Med. 2001;6(3 Suppl):3–7. - PubMed
-
- Meijer WT, Hoes AW, Rutgers D, Bots ML, Hofman A, Grobbee DE. Peripheral arterial disease in the elderly: the Rotterdam study. Arterioscler Thromb Vasc Biol. 1998;18(2):185–192. - PubMed
-
- Diehm C, Schuster A, Allenberg JR, et al. High prevalence of peripheral arterial disease and comorbidity in 6880 primary care patients: cross-sectional study. Atherosclerosis. 2004;172(1):95–105. - PubMed
-
- Hirsch AT, Criqui MH, Treat-Jacobson D, et al. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA. 2001;286(11):1317–1324. - PubMed
-
- Saw J, Bhatt DL, Moliterno DJ, et al. The influence of peripheral arterial disease on outcomes: a pooled analysis of mortality in eight large randomized percutaneous coronary intervention trials. J Am Coll Cardiol. 2006;48(8):1567–1572. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
