

Nevirapine versus ritonavir-boosted lopinavir for HIV-infected children
- PMID: 22716976
- PMCID: PMC3443859
- DOI: 10.1056/NEJMoa1113249
Nevirapine versus ritonavir-boosted lopinavir for HIV-infected children
Abstract
Background: Nevirapine-based antiretroviral therapy is the predominant (and often the only) regimen available for children in resource-limited settings. Nevirapine resistance after exposure to the drug for prevention of maternal-to-child human immunodeficiency virus (HIV) transmission is common, a problem that has led to the recommendation of ritonavir-boosted lopinavir in such settings. Regardless of whether there has been prior exposure to nevirapine, the performance of nevirapine versus ritonavir-boosted lopinavir in young children has not been rigorously established.
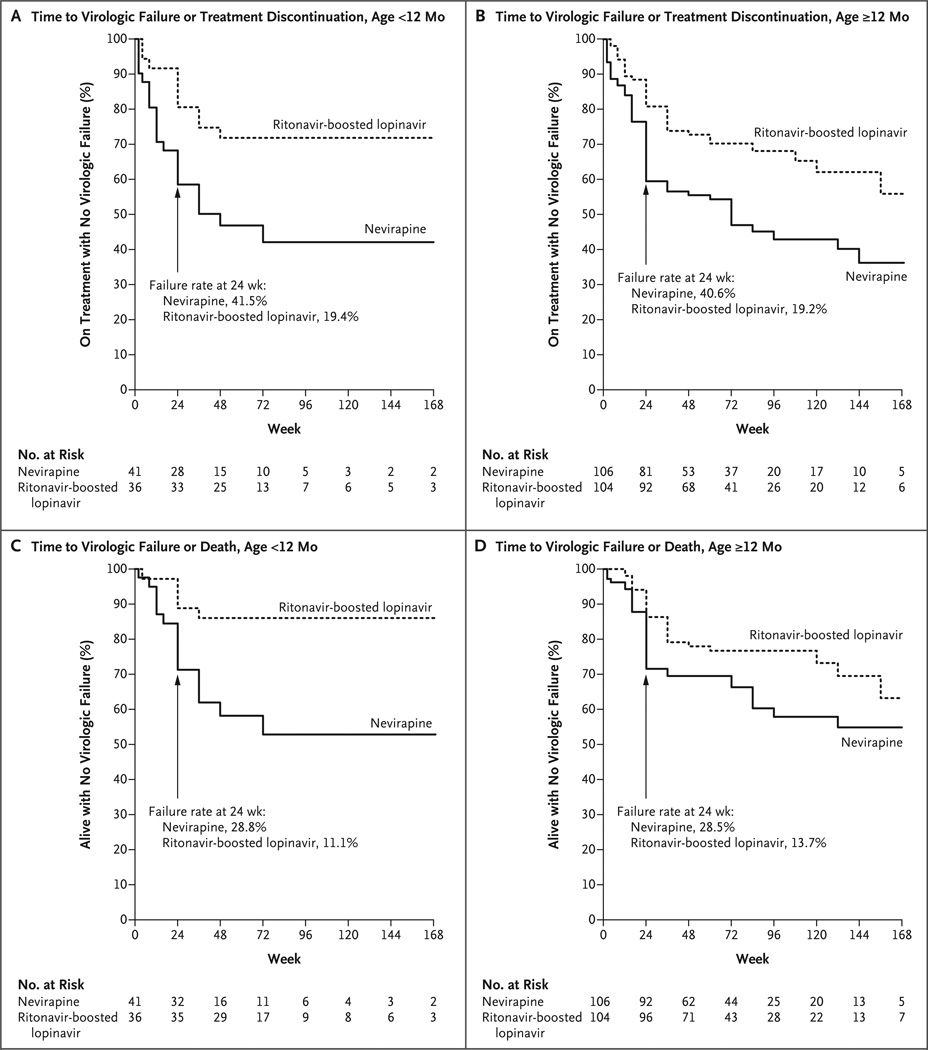
Methods: In a randomized trial conducted in six African countries and India, we compared the initiation of HIV treatment with zidovudine, lamivudine, and either nevirapine or ritonavir-boosted lopinavir in HIV-infected children 2 to 36 months of age who had no prior exposure to nevirapine. The primary end point was virologic failure or discontinuation of treatment by study week 24.
Results: A total of 288 children were enrolled; the median percentage of CD4+ T cells was 15%, and the median plasma HIV type 1 (HIV-1) RNA level was 5.7 log(10) copies per milliliter. The percentage of children who reached the primary end point was significantly higher in the nevirapine group than in the ritonavir-boosted lopinavir group (40.8% vs. 19.3%; P<0.001). Among the nevirapine-treated children with virologic failure for whom data on resistance were available, more than half (19 of 32) had resistance at the time of virologic failure. In addition, the time to a protocol-defined toxicity end point was shorter in the nevirapine group (P=0.04), as was the time to death (P=0.06).
Conclusions: Outcomes were superior with ritonavir-boosted lopinavir among young children with no prior exposure to nevirapine. Factors that may have contributed to the suboptimal results with nevirapine include elevated viral load at baseline, selection for nevirapine resistance, background regimen of nucleoside reverse-transcriptase inhibitors, and the standard ramp-up dosing strategy. The results of this trial present policymakers with difficult choices. (Funded by the National Institute of Allergy and Infectious Diseases and others; P1060 ClinicalTrials.gov number, NCT00307151.).
Conflict of interest statement
Dr. Avy Violari reports receiving lecture fees from Abbott, consulting fees from Tibotec, and trial drugs from GlaxoSmith-Kline; Dr. Hughes, consulting fees from Boehringer Ingelheim, Pfizer, Medicines Development, and Tibotec and support for a scientific workshop from Merck; Dr. Cotton, lecture fees from Abbott; and Dr. Moultrie, grants from GlaxoSmithKline, ViiV Healthcare, and Tibotec. No other potential conflict of interest relevant to this article was reported.
Figures
References
-
- Geneva: World Health Organization Technical Reference Group; 2010. Antiretroviral therapy of HIV infection in infants and children: towards universal access: recommendations for a public health approach — 2010 revision. - PubMed
-
- Babiker A, Castro HG, Compagnucci A, et al. First-line antiretroviral therapy with a protease inhibitor versus non-nucleoside reverse transcriptase inhibitor and switch at higher versus low viral load in HIV-infected children: an open-label, randomized phase 2/3 trial. Lancet Infect Dis. 2011;11:273–283. - PMC - PubMed
-
- Palumbo P, Wu H, Chadwick E, et al. Virologic response to potent antiretroviral therapy and modeling of HIV dynamics in early pediatric infection. J Infect Dis. 2007;196:23–29. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials