

Analysing recent socioeconomic trends in coronary heart disease mortality in England, 2000-2007: a population modelling study
- PMID: 22719232
- PMCID: PMC3373639
- DOI: 10.1371/journal.pmed.1001237
Analysing recent socioeconomic trends in coronary heart disease mortality in England, 2000-2007: a population modelling study
Abstract
Background: Coronary heart disease (CHD) mortality in England fell by approximately 6% every year between 2000 and 2007. However, rates fell differentially between social groups with inequalities actually widening. We sought to describe the extent to which this reduction in CHD mortality was attributable to changes in either levels of risk factors or treatment uptake, both across and within socioeconomic groups.
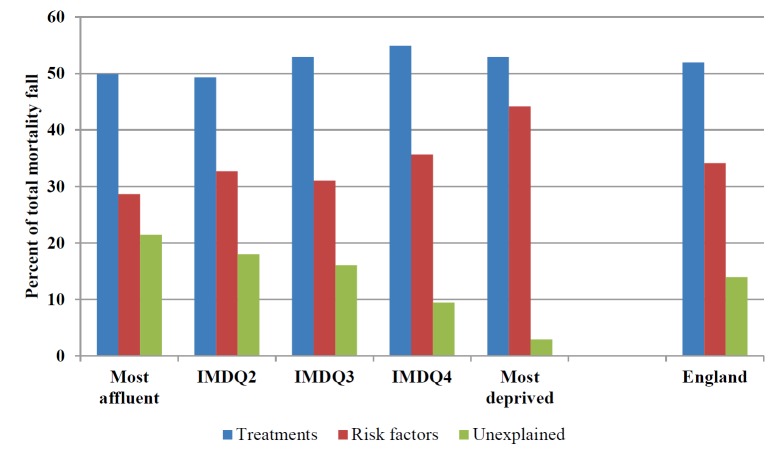
Methods and findings: A widely used and replicated epidemiological model was used to synthesise estimates stratified by age, gender, and area deprivation quintiles for the English population aged 25 and older between 2000 and 2007. Mortality rates fell, with approximately 38,000 fewer CHD deaths in 2007. The model explained about 86% (95% uncertainty interval: 65%-107%) of this mortality fall. Decreases in major cardiovascular risk factors contributed approximately 34% (21%-47%) to the overall decline in CHD mortality: ranging from about 44% (31%-61%) in the most deprived to 29% (16%-42%) in the most affluent quintile. The biggest contribution came from a substantial fall in systolic blood pressure in the population not on hypertension medication (29%; 18%-40%); more so in deprived (37%) than in affluent (25%) areas. Other risk factor contributions were relatively modest across all social groups: total cholesterol (6%), smoking (3%), and physical activity (2%). Furthermore, these benefits were partly negated by mortality increases attributable to rises in body mass index and diabetes (-9%; -17% to -3%), particularly in more deprived quintiles. Treatments accounted for approximately 52% (40%-70%) of the mortality decline, equitably distributed across all social groups. Lipid reduction (14%), chronic angina treatment (13%), and secondary prevention (11%) made the largest medical contributions.
Conclusions: The model suggests that approximately half the recent CHD mortality fall in England was attributable to improved treatment uptake. This benefit occurred evenly across all social groups. However, opposing trends in major risk factors meant that their net contribution amounted to just over a third of the CHD deaths averted; these also varied substantially by socioeconomic group. Powerful and equitable evidence-based population-wide policy interventions exist; these should now be urgently implemented to effectively tackle persistent inequalities.
Conflict of interest statement
The following competing interests have been declared. (1) MB, SS, HL have support from Legal and General Assurance Society Limited for the submitted work; (2) NH, MOF, RR, SC have no relationships with Legal and General Assurance Society Limited that might have an interest in the submitted work in the previous 3 years; (3) their spouses, partners, or children have no financial relationships that may be relevant to the submitted work; and (4) MB, SS, HL, MOF, NH, RR have no nonfinancial interests that may be relevant to the submitted work; SC was a member of the NICE Programme Development Group on CVD Prevention in Populations. However, this article does not necessarily represent the views of NICE. The authors have declared that no other competing interests exist.
Figures
References
-
- Bajekal M, Scholes S, O'Flaherty M, Raine R, Norman P, et al. Trends in CHD mortality by socioeconomic circumstances, England 1982–2006. J Epidemiol Community Health. 2010;64(Suppl 1) p.A2.
-
- The Marmot Review. Fair society, healthy lives: strategic review of health inequalities in England post-2010. 2010. London: The Marmot Review, Available: http://www.instituteofhealthequity.org/projects/fair-society-healthy-liv....
-
- Unal B, Critchley JA, Capewell S. Explaining the decline in coronary heart disease mortality in England and Wales between 1981 and 2000. Circulation. 2004;109:1101–1107. - PubMed
-
- Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, et al. Explaining the decrease in US deaths from coronary disease, 1980–2000. N Engl J Med. 2007;356:2388–2398. Detailed technical appendix of model available available: http://www.nejm.org/doi/suppl/10.1056/NEJMsa053935/suppl_file/nejm_ford_.... - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
