

A multifaceted intervention to improve the quality of care of children in district hospitals in Kenya: a cost-effectiveness analysis
- PMID: 22719233
- PMCID: PMC3373608
- DOI: 10.1371/journal.pmed.1001238
A multifaceted intervention to improve the quality of care of children in district hospitals in Kenya: a cost-effectiveness analysis
Abstract
Background: To improve care for children in district hospitals in Kenya, a multifaceted approach employing guidelines, training, supervision, feedback, and facilitation was developed, for brevity called the Emergency Triage and Treatment Plus (ETAT+) strategy. We assessed the cost effectiveness of the ETAT+ strategy, in Kenyan hospitals. Further, we estimate the costs of scaling up the intervention to Kenya nationally and potential cost effectiveness at scale.
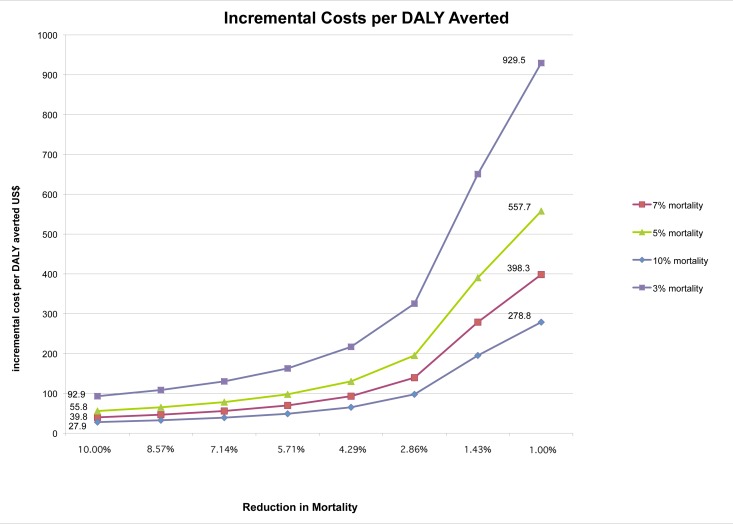
Methods and findings: Our cost-effectiveness analysis from the provider's perspective used data from a previously reported cluster randomized trial comparing the full ETAT+ strategy (n = 4 hospitals) with a partial intervention (n = 4 hospitals). Effectiveness was measured using 14 process measures that capture improvements in quality of care; their average was used as a summary measure of quality. Economic costs of the development and implementation of the intervention were determined (2009 US$). Incremental cost-effectiveness ratios were defined as the incremental cost per percentage improvement in (average) quality of care. Probabilistic sensitivity analysis was used to assess uncertainty. The cost per child admission was US$50.74 (95% CI 49.26-67.06) in intervention hospitals compared to US$31.1 (95% CI 30.67-47.18) in control hospitals. Each percentage improvement in average quality of care cost an additional US$0.79 (95% CI 0.19-2.31) per admitted child. The estimated annual cost of nationally scaling up the full intervention was US$3.6 million, approximately 0.6% of the annual child health budget in Kenya. A "what-if" analysis assuming conservative reductions in mortality suggests the incremental cost per disability adjusted life year (DALY) averted by scaling up would vary between US$39.8 and US$398.3.
Conclusion: Improving quality of care at scale nationally with the full ETAT+ strategy may be affordable for low income countries such as Kenya. Resultant plausible reductions in hospital mortality suggest the intervention could be cost-effective when compared to incremental cost-effectiveness ratios of other priority child health interventions.
Conflict of interest statement
ME was responsible for developing the intervention that is the subject of the cost-effectiveness analysis and testing its implementation. All other authors have declared that no competing interests exist.
Figures
References
-
- UNICEF. Levels and trends in child mortality. New York: UNICEF; 2011.
-
- You D, Wardlaw T, Salama P, Jones G. Levels and trends in under-5 mortality, 1990–2008. Lancet. 2009;375:100–103. - PubMed
-
- Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS. How many child deaths can we prevent this year? Lancet. 2003;362:65–71. - PubMed
-
- Claeson M, Gillespie D, Mshinda H, Troedsson H, Victora CG. Knowledge into action for child survival. Lancet. 2003;362:323–327. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
