

Implementing the global plan to stop TB, 2011-2015--optimizing allocations and the Global Fund's contribution: a scenario projections study
- PMID: 22719954
- PMCID: PMC3377722
- DOI: 10.1371/journal.pone.0038816
Implementing the global plan to stop TB, 2011-2015--optimizing allocations and the Global Fund's contribution: a scenario projections study
Abstract
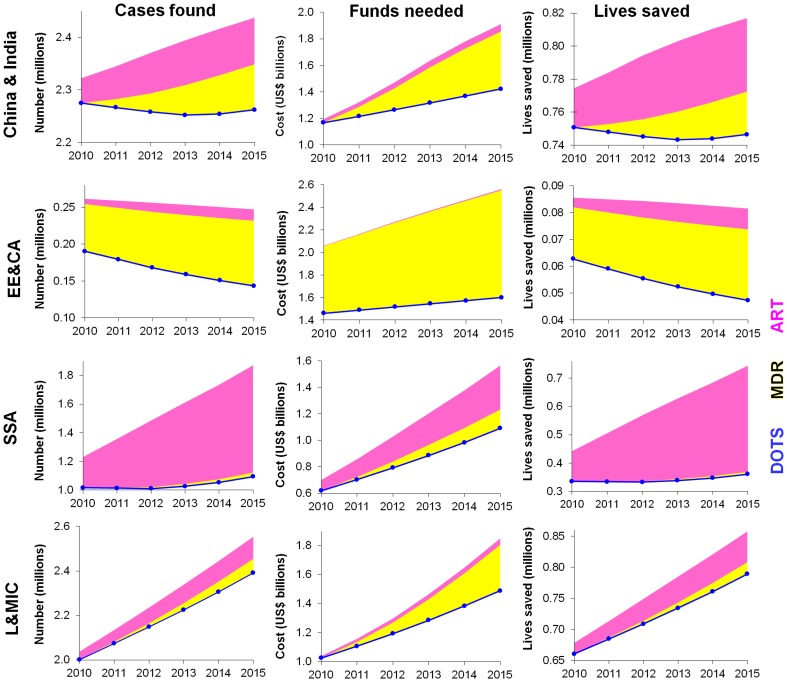
Background: The Global Plan to Stop TB estimates funding required in low- and middle-income countries to achieve TB control targets set by the Stop TB Partnership within the context of the Millennium Development Goals. We estimate the contribution and impact of Global Fund investments under various scenarios of allocations across interventions and regions.
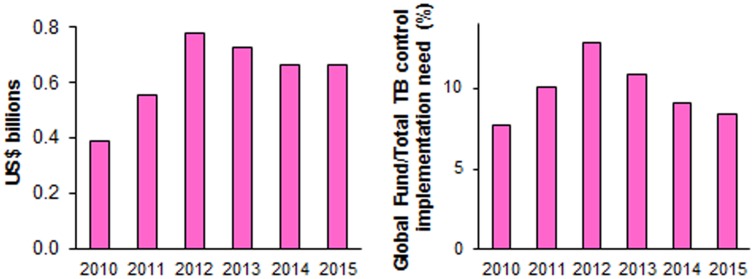
Methodology/principal findings: Using Global Plan assumptions on expected cases and mortality, we estimate treatment costs and mortality impact for diagnosis and treatment for drug-sensitive and multidrug-resistant TB (MDR-TB), including antiretroviral treatment (ART) during DOTS for HIV-co-infected patients, for four country groups, overall and for the Global Fund investments. In 2015, China and India account for 24% of funding need, Eastern Europe and Central Asia (EECA) for 33%, sub-Saharan Africa (SSA) for 20%, and other low- and middle-income countries for 24%. Scale-up of MDR-TB treatment, especially in EECA, drives an increasing global TB funding need--an essential investment to contain the mortality burden associated with MDR-TB and future disease costs. Funding needs rise fastest in SSA, reflecting increasing coverage need of improved TB/HIV management, which saves most lives per dollar spent in the short term. The Global Fund is expected to finance 8-12% of Global Plan implementation costs annually. Lives saved through Global Fund TB support within the available funding envelope could increase 37% if allocations shifted from current regional demand patterns to a prioritized scale-up of improved TB/HIV treatment and secondly DOTS, both mainly in Africa--with EECA region, which has disproportionately high per-patient costs, funded from alternative resources.
Conclusions/significance: These findings, alongside country funding gaps, domestic funding and implementation capacity and equity considerations, should inform strategies and policies for international donors, national governments and disease control programs to implement a more optimal investment approach focusing on highest-impact populations and interventions.
Conflict of interest statement
Figures

Similar articles
-
Financial resources required for tuberculosis control to achieve global targets set for 2015.Bull World Health Organ. 2008 Jul;86(7):568-76. doi: 10.2471/blt.07.049767. Bull World Health Organ. 2008. PMID: 18670669 Free PMC article.
-
Fighting the tuberculosis epidemic in the Western Pacific region: current situation and challenges ahead.Kekkaku. 2010 Jan;85(1):9-16. Kekkaku. 2010. PMID: 20143671
-
Global Fund investments in human resources for health: innovation and missed opportunities for health systems strengthening.Health Policy Plan. 2014 Dec;29(8):986-97. doi: 10.1093/heapol/czt080. Epub 2013 Nov 6. Health Policy Plan. 2014. PMID: 24197405
-
[Fight against tuberculosis in the world].Rev Pneumol Clin. 2015 Apr-Jun;71(2-3):181-7. doi: 10.1016/j.pneumo.2014.03.004. Epub 2014 May 28. Rev Pneumol Clin. 2015. PMID: 24878188 Review. French.
-
Global epidemiology of tuberculosis.Semin Respir Crit Care Med. 2013 Feb;34(1):3-16. doi: 10.1055/s-0032-1333467. Epub 2013 Mar 4. Semin Respir Crit Care Med. 2013. PMID: 23460002 Review.
Cited by
-
MDR-TB treatment as prevention: The projected population-level impact of expanded treatment for multidrug-resistant tuberculosis.PLoS One. 2017 Mar 8;12(3):e0172748. doi: 10.1371/journal.pone.0172748. eCollection 2017. PLoS One. 2017. PMID: 28273116 Free PMC article.
-
Antiretroviral Treatment Scale-Up and Tuberculosis Mortality in High TB/HIV Burden Countries: An Econometric Analysis.PLoS One. 2016 Aug 18;11(8):e0160481. doi: 10.1371/journal.pone.0160481. eCollection 2016. PLoS One. 2016. PMID: 27536864 Free PMC article.
-
Prevalence of Pulmonary Tuberculosis and Rifampicin Resistance Among Patients Attending Adama Hospital Medical College.Int J Microbiol. 2025 Feb 12;2025:1475396. doi: 10.1155/ijm/1475396. eCollection 2025. Int J Microbiol. 2025. PMID: 39974279 Free PMC article.
-
Factors Associated with Non-Adherence for Prescribed Treatment in 201 Patients with Multidrug-Resistant and Rifampicin-Resistant Tuberculosis in Anhui Province, China.Med Sci Monit. 2022 Apr 19;28:e935334. doi: 10.12659/MSM.935334. Med Sci Monit. 2022. PMID: 35437301 Free PMC article.
-
TLR1 polymorphisms are significantly associated with the occurrence, presentation and drug-adverse reactions of tuberculosis in Western Chinese adults.Oncotarget. 2017 Dec 8;9(2):1691-1704. doi: 10.18632/oncotarget.23067. eCollection 2018 Jan 5. Oncotarget. 2017. PMID: 29416723 Free PMC article.
References
-
- Stop TB Partnership World Health Organization. The Global Plan to Stop TB 2011–2015: Transforming the fight towards elimination of tuberculosis. Geneva: Stop TB Partnership. 2010.
-
- The Global Fund to fight AIDS Tuberculosis Malaria. Global Fund-supported programs see strong results amid funding challenges [press release]. Geneva. 2011.
-
- World Health Organization. Global tuberculosis control 2011. 2011.
-
- The Global Fund to fight AIDS Tuberculosis Malaria. Approved Grant Amounts and Disbursements: Disbursements in detail, Commitments and disbursements – summary. 2012.
-
- Kazatchkine MD. Increased resources for the Global Fund, but pledges fall short of expected demand. Lancet. 2010;376:1439–1440. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
