

Evaluation of a multiparametric immunofluorescence assay for standardization of neuromyelitis optica serology
- PMID: 22719979
- PMCID: PMC3373605
- DOI: 10.1371/journal.pone.0038896
Evaluation of a multiparametric immunofluorescence assay for standardization of neuromyelitis optica serology
Abstract
Background: Neuromyelitis optica (NMO) is a severely disabling autoimmune disorder of the central nervous system, which predominantly affects the optic nerves and spinal cord. In a majority of cases, NMO is associated with antibodies to aquaporin-4 (AQP4) (termed NMO-IgG).
Aims: In this study, we evaluated a new multiparametric indirect immunofluorescence (IIF) assay for NMO serology.
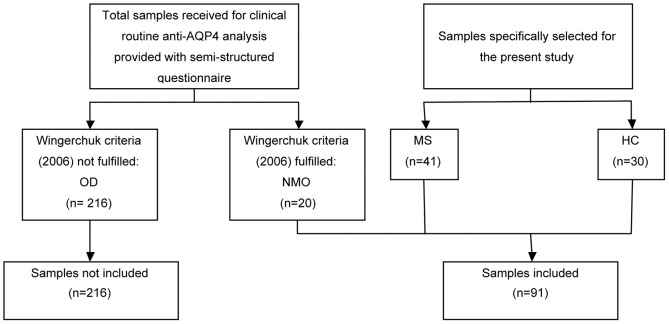
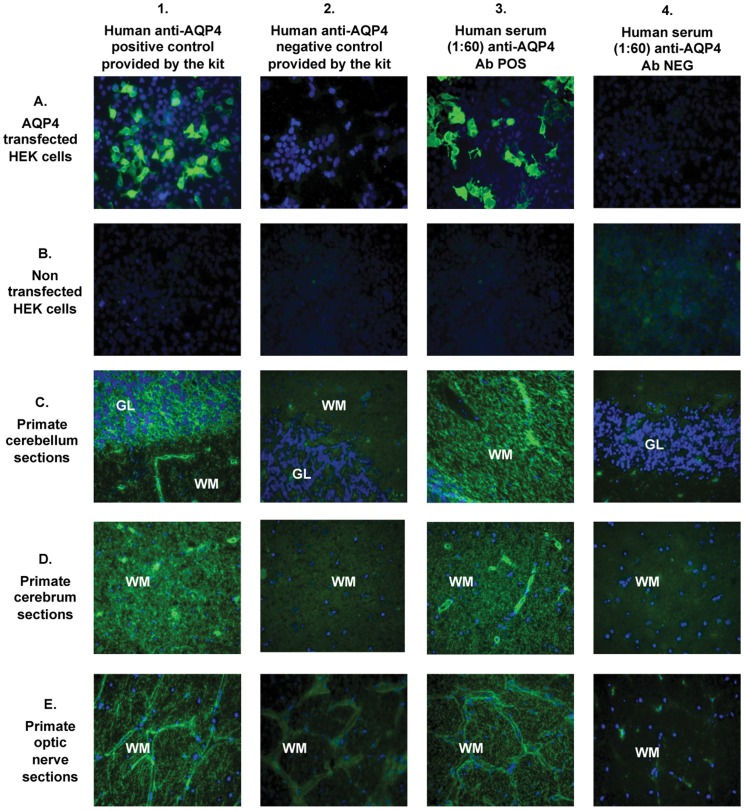
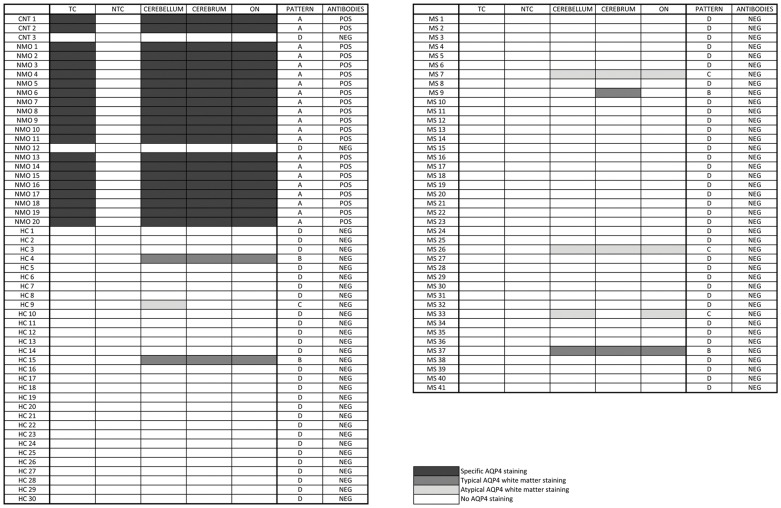
Methods: Sera from 20 patients with NMO, 41 patients with multiple sclerosis (MS), 30 healthy subjects, and a commercial anti-AQP4 IgG antibody were tested in a commercial composite immunofluorescence assay ("Neurology Mosaic 17"; Euroimmun, Germany), consisting of five different diagnostic substrates (HEK cells transfected with AQP4, non-transfected HEK cells, primate cerebellum, cerebrum, and optic nerve tissue sections).
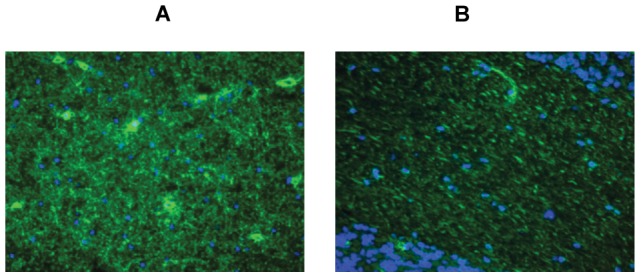
Results: We identified AQP4 specific and non-specific fluorescence staining patterns and established positivity criteria. Based on these criteria, this kit yielded a high sensitivity (95%) and specificity (100%) for NMO and had a significant positive and negative likelihood ratio (LR+ = ∞, LR- = 0.05). Moreover, a 100% inter- and intra-laboratory reproducibility was found.
Conclusions: The biochip mosaic assay tested in this study is a powerful tool for NMO serology, fast to perform, highly sensitive and specific for NMO, reproducible, and suitable for inter-laboratory standardization as required for multi-centre clinical trials.
Conflict of interest statement
Figures
References
-
- Wingerchuk DM, Hogancamp WF, O'Brien PC, Weinshenker BG. The clinical course of neuromyelitis optica (Devic's syndrome). Neurology. 1999;53(5):1107–1114. - PubMed
-
- Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica. Neurology 23: 66(10),1485–1489. 2006. - PubMed
-
- Lennon VA, Wingerchuk DM, Kryzer TJ, Pittock SJ, Lucchinetti CF, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet. 2004;364:2106–2112. - PubMed
-
- Weinshenker BG, Wingerchuk DM, Vukusic S, Linbo L, Pittock SJ, et al. Neuromyelitis optica IgG predicts relapse after longitudinally extensive transverse myelitis. Ann Neurol. 2006;59:566–569. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
