

Microglial activation correlates with disease progression and upper motor neuron clinical symptoms in amyotrophic lateral sclerosis
- PMID: 22720079
- PMCID: PMC3375234
- DOI: 10.1371/journal.pone.0039216
Microglial activation correlates with disease progression and upper motor neuron clinical symptoms in amyotrophic lateral sclerosis
Abstract
Background/aims: We evaluated clinicopathological correlates of upper motor neuron (UMN) damage in amyotrophic lateral sclerosis (ALS), and analyzed if the presence of the C9ORF72 repeat expansion was associated with alterations in microglial inflammatory activity.
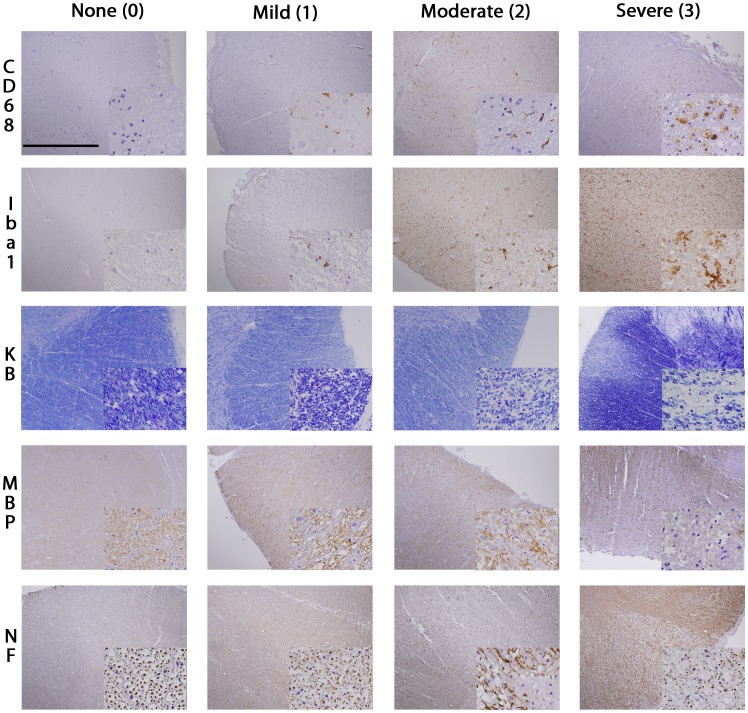
Methods: Microglial pathology was assessed by IHC with 2 different antibodies (CD68, Iba1), myelin loss by Kluver-Barrera staining and myelin basic protein (MBP) IHC, and axonal loss by neurofilament protein (TA51) IHC, performed on 59 autopsy cases of ALS including 9 cases with C9ORF72 repeat expansion.
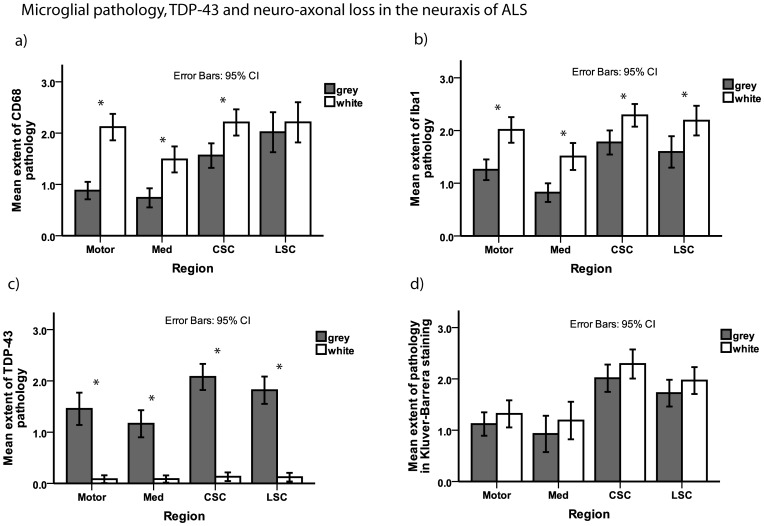
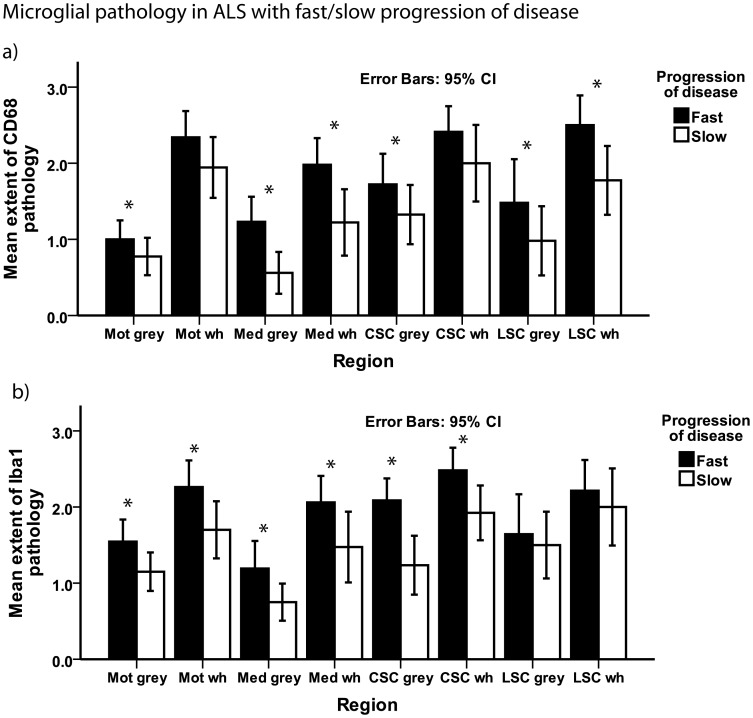
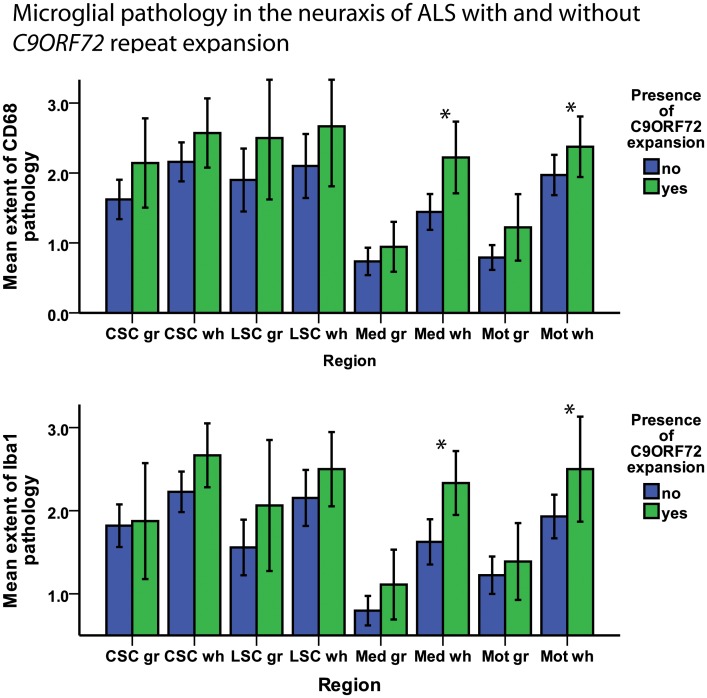
Results: Microglial pathology as depicted by CD68 and Iba1 was significantly more extensive in the corticospinal tract (CST) of ALS cases with a rapid progression of disease. Cases with C9ORF72 repeat expansion showed more extensive microglial pathology in the medulla and motor cortex which persisted after adjusting for disease duration in a logistic regression model. Higher scores on the clinical UMN scale correlated with increasing microglial pathology in the cervical CST. TDP-43 pathology was more extensive in the motor cortex of cases with rapid progression of disease.
Conclusions: This study demonstrates that microglial pathology in the CST of ALS correlates with disease progression and is linked to severity of UMN deficits.
Conflict of interest statement
Figures
References
-
- Kiernan MC, Vucic S, Cheah BC, Turner MR, Eisen A, et al. Amyotrophic lateral sclerosis. Lancet. 2011;377:942–955. - PubMed
-
- Neumann M, Sampathu DM, Kwong LK, Truax AC, Micsenyi MC, et al. Ubiquitinated TDP-43 in frontotemporal lobar degeneration and amyotrophic lateral sclerosis. Science. 2006;314:130–133. - PubMed
-
- Deng HX, Hentati A, Tainer JA, Iqbal Z, Cayabyab A, et al. Amyotrophic lateral sclerosis and structural defects in Cu,Zn superoxide dismutase. Science. 1993;261:1047–1051. - PubMed
-
- Pehar M, Cassina P, Vargas MR, Castellanos R, Viera L, et al. Astrocytic production of nerve growth factor in motor neuron apoptosis: implications for amyotrophic lateral sclerosis. J Neurochem. 2004;89:464–473. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
