

doi: 10.4253/wjge.v4.i6.247.
Pancreatic cystic lesions: How endoscopic ultrasound morphology and endoscopic ultrasound fine needle aspiration help unlock the diagnostic puzzle
Affiliations
- PMID: 22720127
- PMCID: PMC3377868
- DOI: 10.4253/wjge.v4.i6.247
Item in Clipboard
Pancreatic cystic lesions: How endoscopic ultrasound morphology and endoscopic ultrasound fine needle aspiration help unlock the diagnostic puzzle
World J Gastrointest Endosc.
.
Abstract
Cystic lesions of the pancreas are being diagnosed with increasing frequency, covering a vast spectrum from benign to malignant and invasive lesions. Numerous investigations can be done to discriminate between benign and non-evolutive lesions from those that require surgery. At the moment, there is no single test that will allow a correct diagnosis in all cases. Endoscopic ultrasound (EUS) morphology, cyst fluid analysis and cytohistology with EUS-guided fine needle aspiration can aid in this difficult diagnosis.
Keywords: Endoscopic ultrasound; Endoscopic ultrasound fine needle aspiration; Pancreatic cystic lesions.
Figures
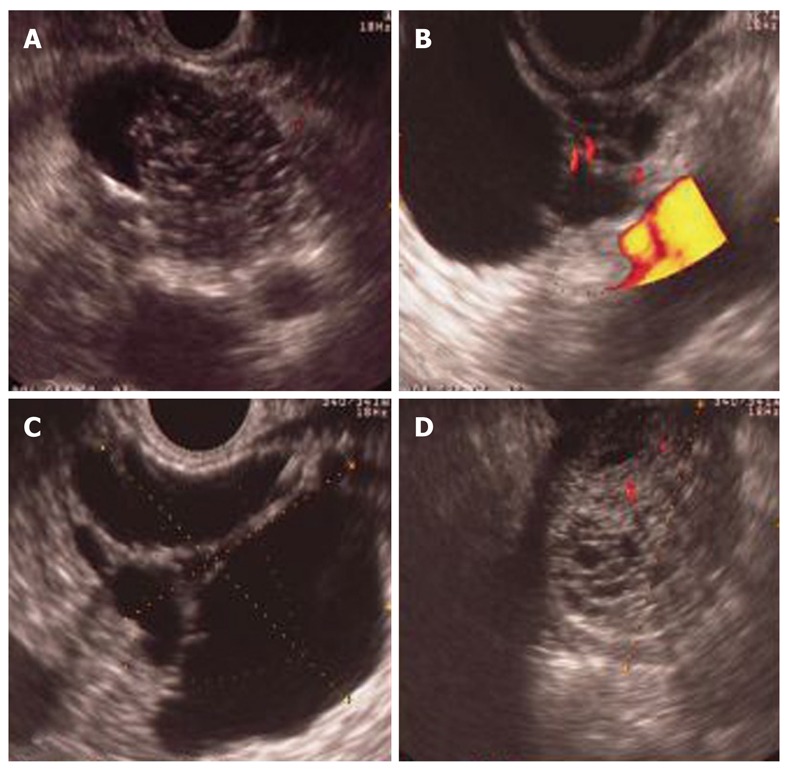
Serous cystoadenoma. A: Microcystic area, centrally located; B: Beside microcystic area; C: Peripheral and internal septa microcystic area, lobulate contour; D: Pseudosolid form.
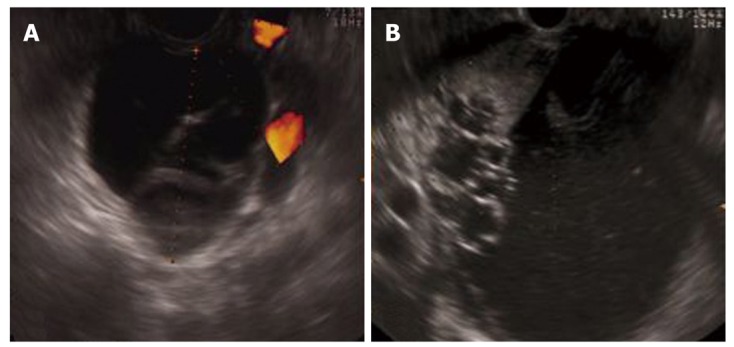
Mucinous cystic neoplasm. A-B: Round lesions with septa (aspects of cysts in cyst with round contour).

Branch duct intraductal papillary mucinous neoplasm. A: “Bunch of grapes” lesion (cysts by cyst aspects with irregular contour); B: Finger-like aspect; C: Clubbed-like aspect.

Pancreatic pseudocyst. Round lesion without septa and with visible hyperechoic debris inside.
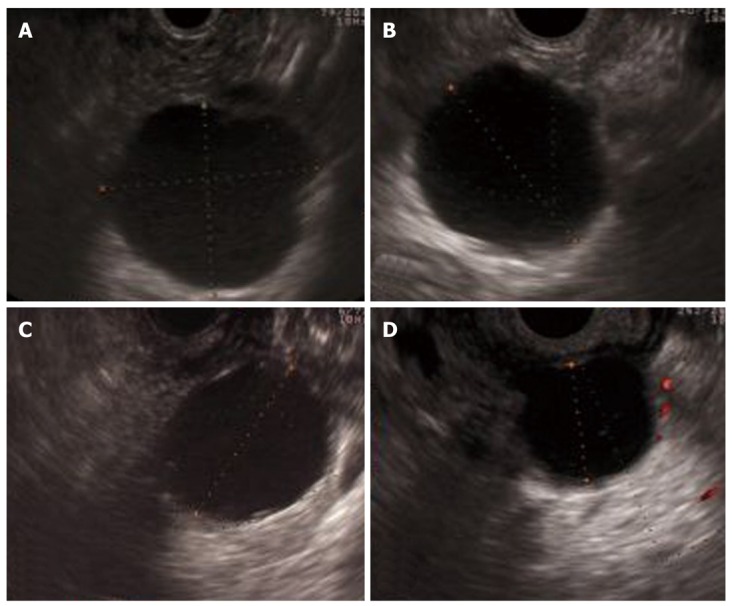
Unilocular aspects in cystic pancreatic lesions. A: Sixty year old female, no symptoms. Lesion in pancreatic head, no visible communication with pancreatic duct. Carcinoembryonic antigen (CEA) 1.5 ng/mL, Amylase 125 U/L, K-RAS mutations negative. Cytology: Cuboidal cell periodic acid-Schiff positive, no mucus. Diagnosis: Unilocular serous cystoadenoma; B: Seventy-nine year old female, no symptoms. Multiple cystic lesion in pancreatic head and tail. Lesion in pancreatic tail with visible communication with pancreatic duct. CEA 12 000 ng/mL, amylase 12 870 U/L, K-RAS mutation positive. Cytology: Mucin and cuboidal cell with mild atypia and papillary arrangement. Diagnosis: Multifocal branch ducts-intraductal papillary mucinous neoplasm; C: Fifty year old female. Lesion in pancreatic body, no visible communication with pancreatic duct. CEA 280 ng/mL, amylase > 15 000 U/L, K-RAS mutation positive. Cytology: Acellular without mucin. Surgical histology: Mucinous cystoadenoma; D: Forty-five year old male, history of alcoholism and recurrent acute pancreatitis. Lesion in pancreatic body. CEA 61 ng/mL, amylase > 15 000 U/L, K-RAS mutations negative. Cytology: Inflammatory cells and pigmented histocytes. Diagnosis: Pancreatic pseudocyst.
References
-
- Kimura W, Nagai H, Kuroda A, Muto T, Esaki Y. Analysis of small cystic lesions of the pancreas. Int J Pancreatol. 1995;18:197–206. - PubMed
-
- Brugge WR, Lauwers GY, Sahani D, Fernandez-del Castillo C, Warshaw AL. Cystic neoplasms of the pancreas. N Engl J Med. 2004;351:1218–1226. - PubMed
-
- Zhang XM, Mitchell DG, Dohke M, Holland GA, Parker L. Pancreatic cysts: depiction on single-shot fast spin-echo MR images. Radiology. 2002;223:547–553. - PubMed
LinkOut - more resources
Full Text Sources
