

Case Reports
doi: 10.1097/MAO.0b013e318254ed98.
Spontaneous intracranial hypotension presenting with severe sensorineural hearing loss and headache
Affiliations
- PMID: 22722142
- PMCID: PMC3600858
- DOI: 10.1097/MAO.0b013e318254ed98
Item in Clipboard
Case Reports
Spontaneous intracranial hypotension presenting with severe sensorineural hearing loss and headache
Otol Neurotol.
2012 Oct.
No abstract available
Conflict of interest statement
The authors disclose no conflicts of interest.
Figures
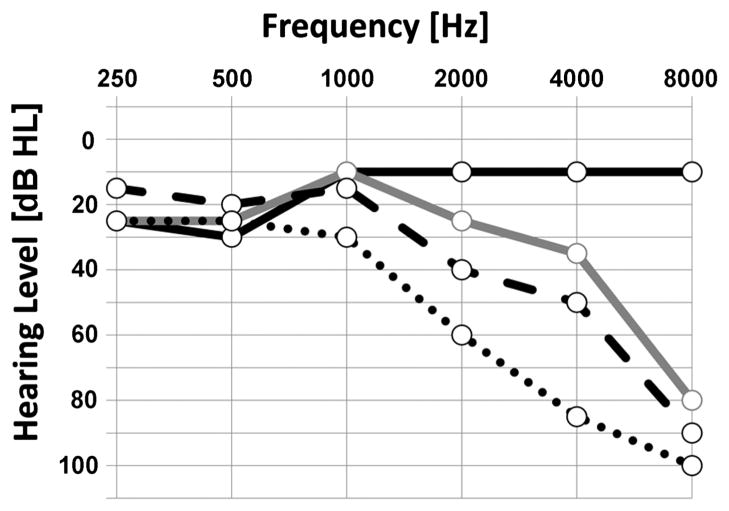
Serial audiograms demonstrate progressive right sensorineural hearing loss for 4 years’ time. Black solid line indicates audiogram from 2007; gray solid line, 2008; dashed line, 2009; dotted line, 2010. Right word recognition scores were 100% until 2010, when it dropped to 92%. Acoustic reflexes were absent in the right ear in all audiograms obtained.
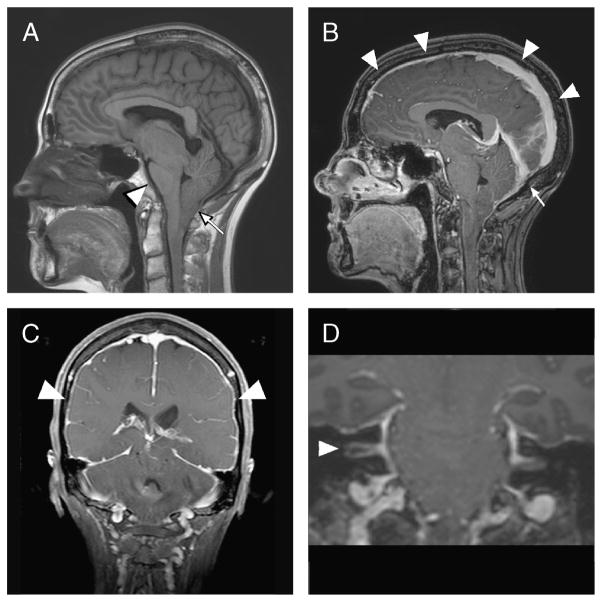
A, Sagittal T1-weighted magnetic resonance image from 2010 demonstrates caudal displacement of intracranial contents, including descent of the cerebellar tonsils with crowding of the foramen magnum (arrow) and flattening of the ventral pons against the clivus (arrowhead). B, Sagittal T1-weighted magnetic resonance image with gadolinium demonstrating prominent sagittal sinus (arrowheads) and transverse sinus (arrow). C, Coronal T1-weighted magnetic resonance image with contrast demonstrating diffuse dural enhancement (arrowheads). D, Coronal T1-weighted magnetic resonance image with contrast showing prominent enhancement resulting from venous engorgement of the porous acousticus of the internal auditory canals, with greater enhancement of the right internal auditory canal (arrowhead) than the left. No mass lesions are present within the internal auditory canals or cerebellopontine angles.
References
-
- Schievink WI. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. JAMA. 2006;295:2286–96. - PubMed
-
- Miller RS, Tami TA, Pensak M. Spontaneous intracranial hypotension mimicking Ménière’s disease. Otolaryngol Head Neck Surg. 2006;135:655–6. - PubMed
-
- Blank SC, Shakir RA, Bindoff LA, et al. Spontaneous intracranial hypotension: clinical and magnetic resonance imaging characteristics. Clin Neurol Neurosurg. 1997;99:199–204. - PubMed
-
- Chung SJ, Kim JS, Lee MC. Syndrome of cerebral spinal fluid hypovolemia: clinical and imaging features and outcome. Neurology. 2000;55:1321–7. - PubMed
-
- Taki M, Nin F, Hasegawa T, et al. Case report: two cases of hearing impairment due to intracranial hypotension. Auris Nasus Larynx. 2009;36:345–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
