

The shrunken, bright cerebellum: a characteristic MRI finding in congenital disorders of glycosylation type 1a
- PMID: 22723063
- PMCID: PMC7965601
- DOI: 10.3174/ajnr.A3151
The shrunken, bright cerebellum: a characteristic MRI finding in congenital disorders of glycosylation type 1a
Abstract
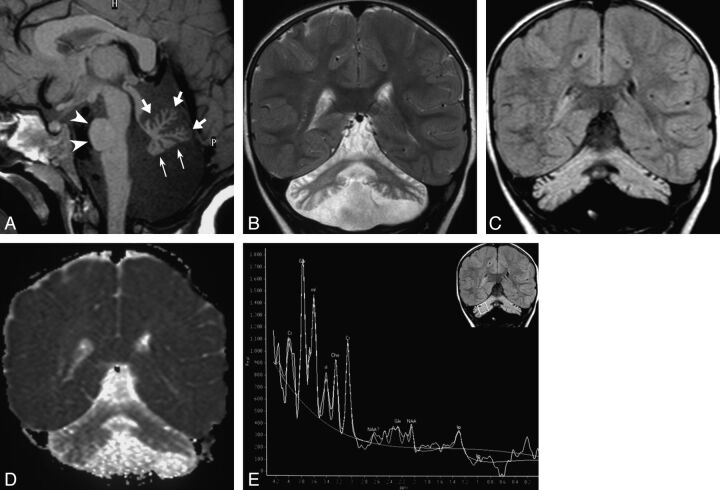
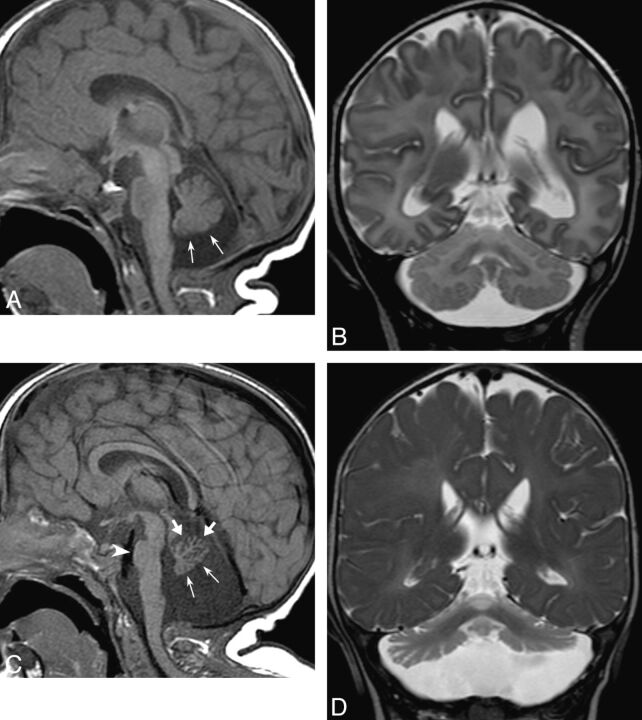
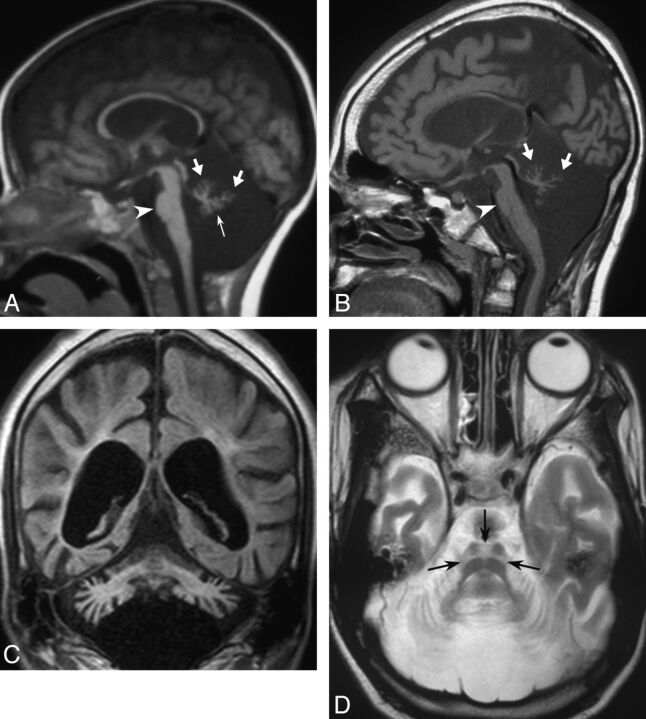
CDG-1a is an early-onset neurodegenerative disease with selective hindbrain involvement and highly variable clinical presentation. We retrospectively reviewed the clinical records and MR imaging studies of 5 children (3 boys and 2 girls aged 12 days to 2 years at presentation) with molecularly confirmed CDG-1a. The cerebellum was hypoplastic at presentation in 4 cases, progressive bulk loss involved the cerebellum and the pons in all cases, and the cerebellar cortex and subcortical white matter were hyperintense on T2-weighted and FLAIR images in all. We conclude that CDG-1a likely results from a combination of cerebellar hypoplasia and atrophy. Cerebellar volume loss with diffuse T2/FLAIR hyperintensity seems to be a peculiar association in the field of cerebellar atrophies, and may be useful to address the differential diagnosis.
Figures
References
-
- Jaeken J, Artigas J, Barone R, et al. . Phosphomannomutase deficiency is the main cause of carbohydrate deficient glycoprotein syndrome with type I isoelectrofocusing pattern of serum sialotransferrins. J Inherit Metab Dis 1997; 20: 447– 49 - PubMed
-
- Sparks SE, Krasnewich DM. PMM2-CDG (CDG-Ia). In: Pagon RA, Bird TD, Dolan CR, et al., eds. GeneReviews [Internet]. Seattle: University of Washington; 1993- 2005 Aug 15 [updated 2011 Apr 21].
-
- Pearl PL, Krasnewich D. Neurologic course of congenital disorders of glycosylation. J Child Neurol 2001; 16: 409– 13 - PubMed
-
- Antoun H, Villeneuve N, Gelot A, et al. . Cerebellar atrophy: an important feature of carbohydrate deficient glycoprotein syndrome type 1. Pediatr Radiol 1999; 29: 194– 98 - PubMed
-
- Jensen PR, Hansen FJ, Skovby F. Cerebellar hypoplasia in children with the carbohydrate-deficient glycoprotein syndrome. Neuroradiology 1995; 37: 328– 30 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical