

Improvement in outcomes of clinical islet transplantation: 1999-2010
- PMID: 22723582
- PMCID: PMC3379615
- DOI: 10.2337/dc12-0063
Improvement in outcomes of clinical islet transplantation: 1999-2010
Abstract
Objective: To describe trends of primary efficacy and safety outcomes of islet transplantation in type 1 diabetes recipients with severe hypoglycemia from the Collaborative Islet Transplant Registry (CITR) from 1999 to 2010.
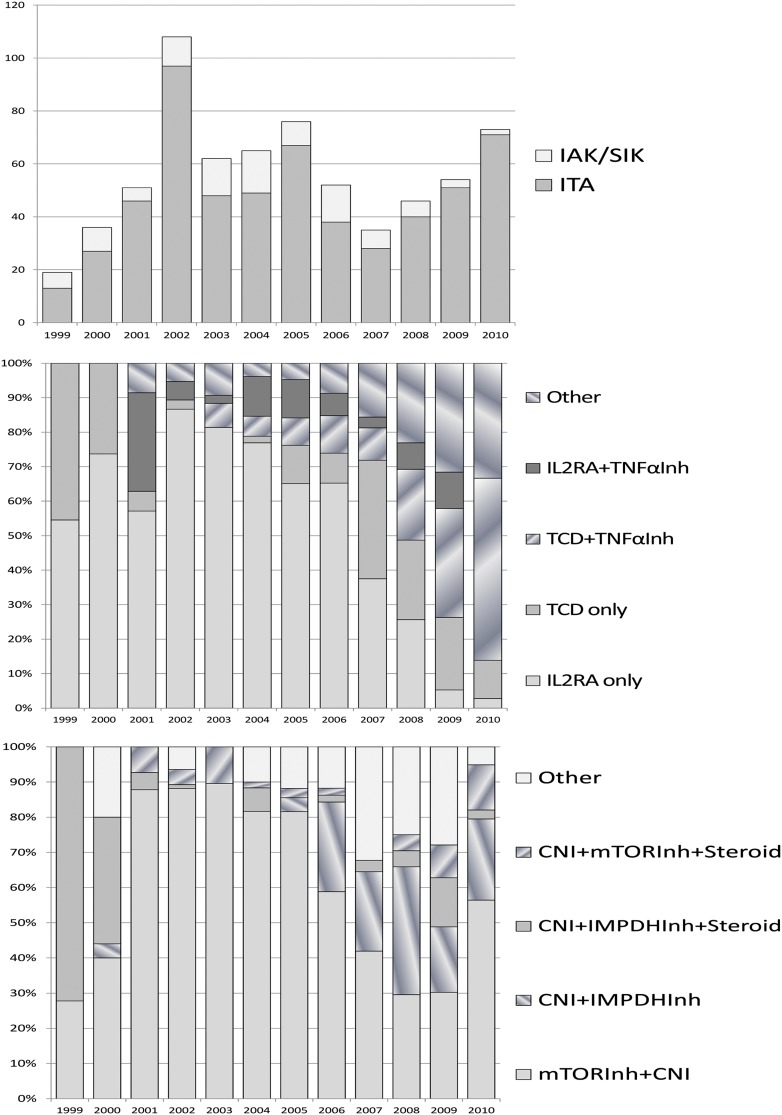
Research design and methods: A total of 677 islet transplant-alone or islet-after-kidney recipients with type 1 diabetes in the CITR were analyzed for five primary efficacy outcomes and overall safety to identify any differences by early (1999-2002), mid (2003-2006), or recent (2007-2010) transplant era based on annual follow-up to 5 years.
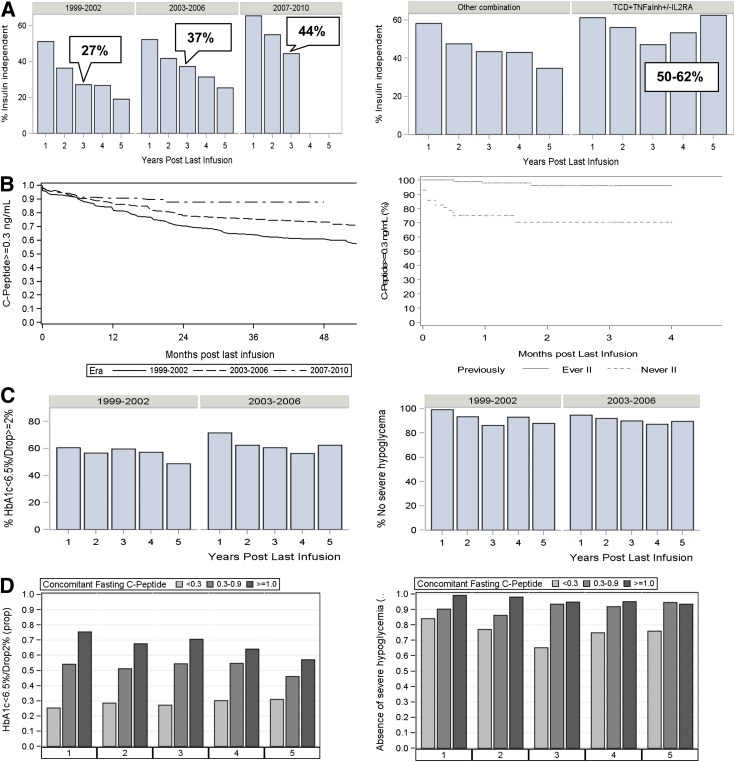
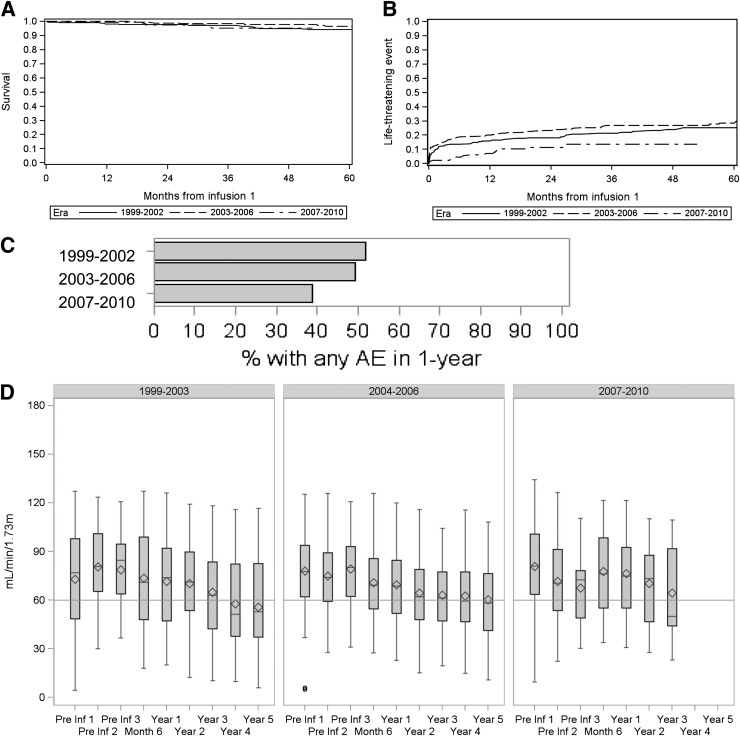
Results: Insulin independence at 3 years after transplant improved from 27% in the early era (1999-2002, n = 214) to 37% in the mid (2003-2006, n = 255) and to 44% in the most recent era (2007-2010, n = 208; P = 0.006 for years-by-era; P = 0.01 for era alone). C-peptide ≥0.3 ng/mL, indicative of islet graft function, was retained longer in the most recent era (P < 0.001). Reduction of HbA(1c) and resolution of severe hypoglycemia exhibited enduring long-term effects. Fasting blood glucose stabilization also showed improvements in the most recent era. There were also modest reductions in the occurrence of adverse events. The islet reinfusion rate was lower: 48% by 1 year in 2007-2010 vs. 60-65% in 1999-2006 (P < 0.01). Recipients that ever achieved insulin-independence experienced longer duration of islet graft function (P < 0.001).
Conclusions: The CITR shows improvement in primary efficacy and safety outcomes of islet transplantation in recipients who received transplants in 2007-2010 compared with those in 1999-2006, with fewer islet infusions and adverse events per recipient.
Figures
References
-
- Hering BJ, Ricordi C. Islet transplantation for patients with type 1 diabetes. Graft 1999;2:12–27
-
- Shapiro AM, Lakey JR, Ryan EA, et al. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N Engl J Med 2000;343:230–238 - PubMed
-
- The Collaborative Islet Transplant Registry (CITR). Seventh Annual Data Report [online report], 2011. Available from http://www.citregistry.org/reports/reports.htm Accessed 9 January 2012
-
- Ryan EA, Shandro T, Green K, et al. Assessment of the severity of hypoglycemia and glycemic lability in type 1 diabetic subjects undergoing islet transplantation. Diabetes 2004;53:955–962 - PubMed
-
- Clinical Islet Transplantation Consortium (CIT) [online]. Available from http://www2.niddk.nih.gov/Research/ScientificAreas/Pancreas/EndocrinePan... Accessed 9 January 2012
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
