

Metabolic disturbances associated with systemic lupus erythematosus
- PMID: 22723834
- PMCID: PMC3378560
- DOI: 10.1371/journal.pone.0037210
Metabolic disturbances associated with systemic lupus erythematosus
Abstract
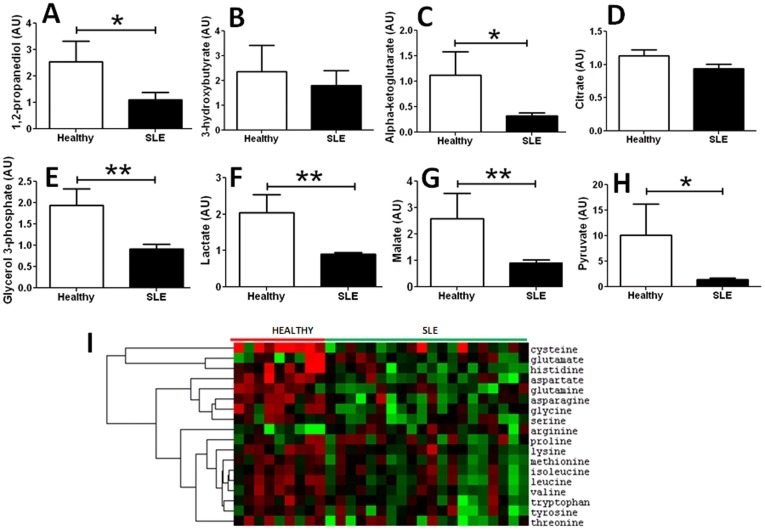
The metabolic disturbances that underlie systemic lupus erythematosus are currently unknown. A metabolomic study was executed, comparing the sera of 20 SLE patients against that of healthy controls, using LC/MS and GC/MS platforms. Validation of key differences was performed using an independent cohort of 38 SLE patients and orthogonal assays. SLE sera showed evidence of profoundly dampened glycolysis, Krebs cycle, fatty acid β oxidation and amino acid metabolism, alluding to reduced energy biogenesis from all sources. Whereas long-chain fatty acids, including the n3 and n6 essential fatty acids, were significantly reduced, medium chain fatty acids and serum free fatty acids were elevated. The SLE metabolome exhibited profound lipid peroxidation, reflective of oxidative damage. Deficiencies were noted in the cellular anti-oxidant, glutathione, and all methyl group donors, including cysteine, methionine, and choline, as well as phosphocholines. The best discriminators of SLE included elevated lipid peroxidation products, MDA, gamma-glutamyl peptides, GGT, leukotriene B4 and 5-HETE. Importantly, similar elevations were not observed in another chronic inflammatory autoimmune disease, rheumatoid arthritis. To sum, comprehensive profiling of the SLE metabolome reveals evidence of heightened oxidative stress, inflammation, reduced energy generation, altered lipid profiles and a pro-thrombotic state. Resetting the SLE metabolome, either by targeting selected molecules or by supplementing the diet with essential fatty acids, vitamins and methyl group donors offers novel opportunities for disease modulation in this disabling systemic autoimmune ailment.
Conflict of interest statement
Figures




References
-
- Deckelbaum RJ. n-6 and n-3 Fatty acids and atherosclerosis: ratios or amounts? Arterioscler Thromb Vasc Biol. 2010;30:2325–2326. - PubMed
-
- Wan JB, Huang LL, Rong R, Tan R, Wang J, et al. Endogenously decreasing tissue n-6/n-3 fatty acid ratio reduces atherosclerotic lesions in apolipoprotein E-deficient mice by inhibiting systemic and vascular inflammation. Arterioscler Thromb Vasc Biol. 2010;30:2487–2494. - PubMed
-
- Nuttall SL, Heaton S, Piper MK, Martin U, Gordon C. Cardiovascular risk in systemic lupus erythematosus–evidence of increased oxidative stress and dyslipidaemia. Rheumatology (Oxford) 2003;42:758–762. - PubMed
-
- Boffa JJ, Rougier JP, Noel N, Ronco P. [High cardiovascular complications in systemic lupus erythematosus: physiopathology and risk management]. Nephrol Ther. 2009;5:595–602. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
