

Apolipoprotein A-II influences apolipoprotein E-linked cardiovascular disease risk in women with high levels of HDL cholesterol and C-reactive protein
- PMID: 22723940
- PMCID: PMC3377620
- DOI: 10.1371/journal.pone.0039110
Apolipoprotein A-II influences apolipoprotein E-linked cardiovascular disease risk in women with high levels of HDL cholesterol and C-reactive protein
Abstract
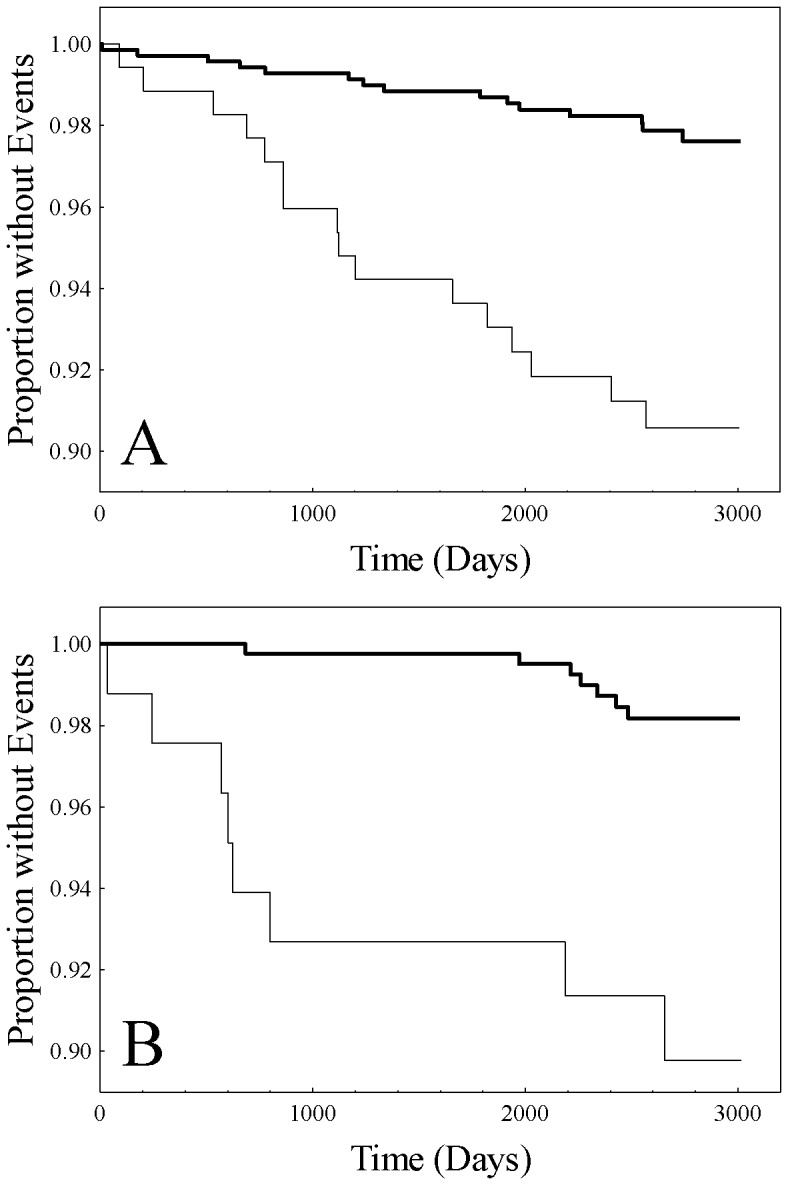
Background: In a previous report by our group, high levels of apolipoprotein E (apoE) were demonstrated to be associated with risk of incident cardiovascular disease in women with high levels of C-reactive protein (CRP) in the setting of both low (designated as HR1 subjects) and high (designated as HR2 subjects) levels of high-density lipoprotein cholesterol (HDL-C). To assess whether apolipoprotein A-II (apoA-II) plays a role in apoE-associated risk in the two female groups.
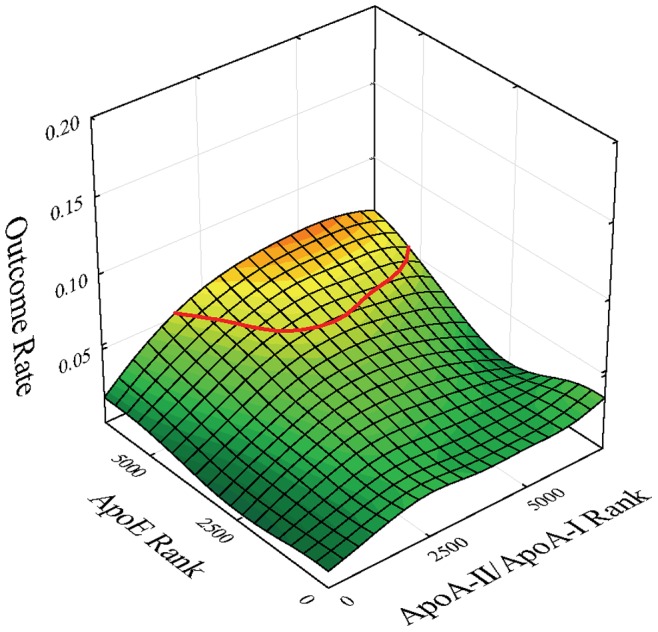
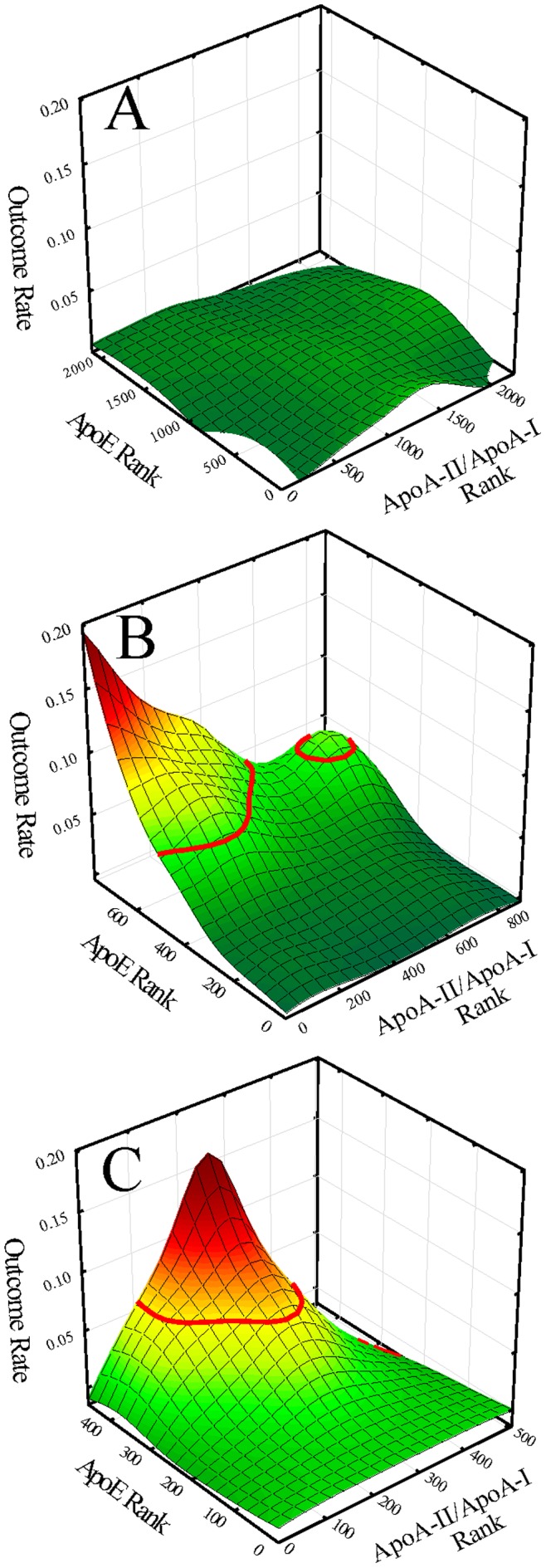
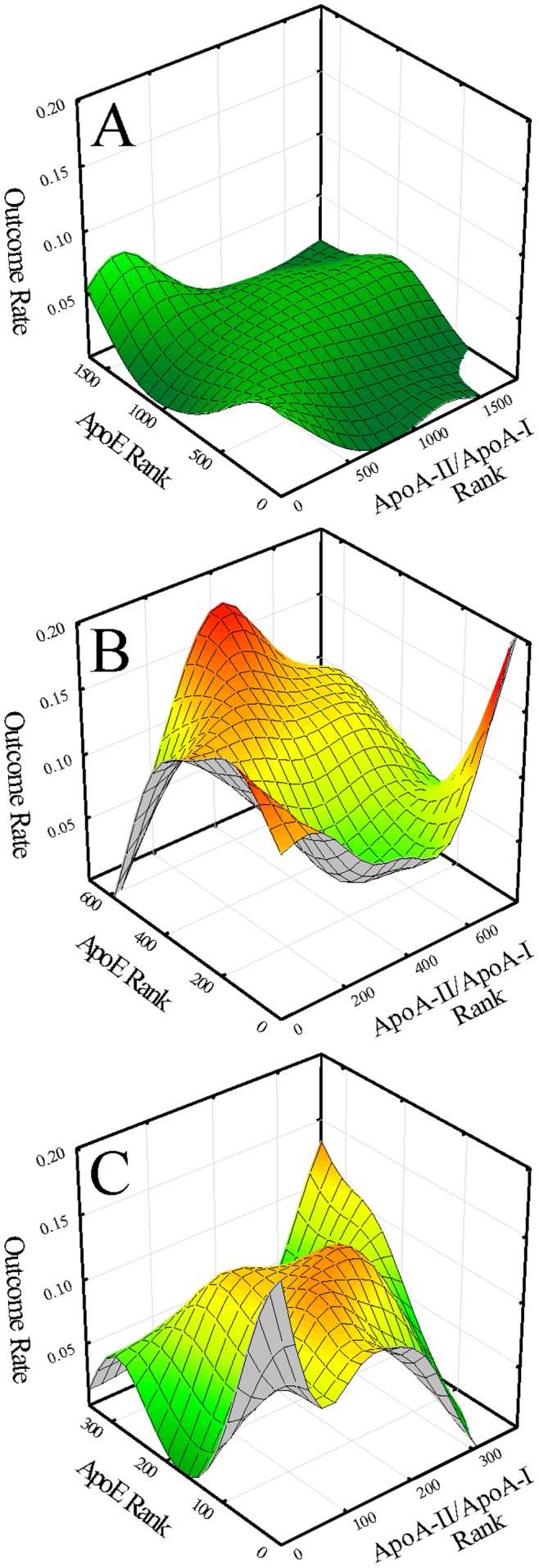
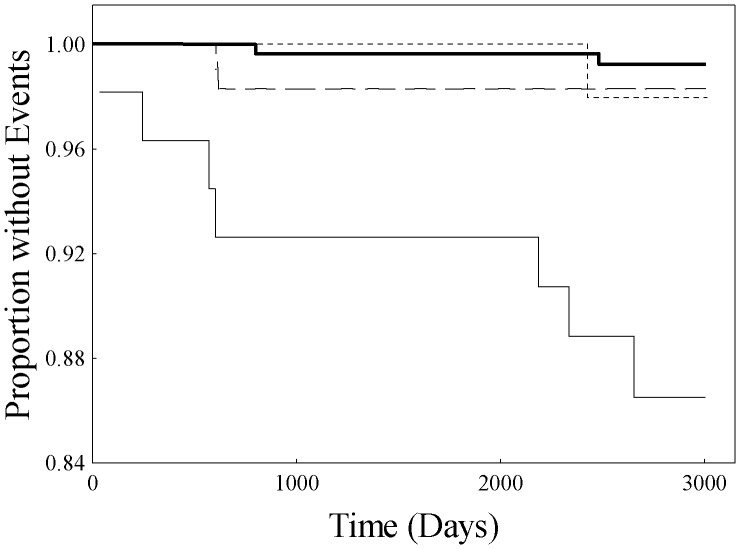
Methodology/principal: Outcome event mapping, a graphical data exploratory tool; Cox proportional hazards multivariable regression; and curve-fitting modeling were used to examine apoA-II influence on apoE-associated risk focusing on HDL particles with apolipoprotein A-I (apoA-I) without apoA-II (LpA-I) and HDL particles with both apoA-I and apoA-II (LpA-I:A-II). Results of outcome mappings as a function of apoE levels and the ratio of apoA-II to apoA-I revealed within each of the two populations, a high-risk subgroup characterized in each situation by high levels of apoE and additionally: in HR1, by a low value of the apoA-II/apoA-I ratio; and in HR2, by a moderate value of the apoA-II/apoA-I ratio. Furthermore, derived estimates of LpA-I and LpA-I:A-II levels revealed for high-risk versus remaining subjects: in HR1, higher levels of LpA-I and lower levels of LpA-I:A-II; and in HR2 the reverse, lower levels of LpA-I and higher levels of LpA-I:A-II. Results of multivariable risk modeling as a function of LpA-I and LpA-I:A-II (dichotomized as highest quartile versus combined three lower quartiles) revealed association of risk only for high levels of LpA-I:A-II in the HR2 subgroup (hazard ratio 5.31, 95% CI 1.12-25.17, p = 0.036). Furthermore, high LpA-I:A-II levels interacted with high apoE levels in establishing subgroup risk.
Conclusions/significance: We conclude that apoA-II plays a significant role in apoE-associated risk of incident CVD in women with high levels of HDL-C and CRP.
Conflict of interest statement
Figures
References
-
- Florentin M, Liberopoulos EN, Wierzbicki AS, Mikhailidis DP. Multiple actions of high-density lipoprotein. Curr Opin Cardiol. 2008;23:370–378. - PubMed
-
- Sviridov D, Mukhamedova N, Remaley AT, Chin-Dusting J, Nestel P. Antiatherogenic functionality of high density lipoprotein: how much versus how good. J Atheroscler Thromb. 2008;15:52–62. - PubMed
-
- Ragbir S, Farmer JA. Dysfunctional high-density lipoprotein and atherosclerosis Curr Atheroscler Rep. 2010;12:343–348. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
