

X-linked genes and risk of orofacial clefts: evidence from two population-based studies in Scandinavia
- PMID: 22723972
- PMCID: PMC3378529
- DOI: 10.1371/journal.pone.0039240
X-linked genes and risk of orofacial clefts: evidence from two population-based studies in Scandinavia
Abstract
Background: Orofacial clefts are common birth defects of complex etiology, with an excess of males among babies with cleft lip and palate, and an excess of females among those with cleft palate only. Although genes on the X chromosome have been implicated in clefting, there has been no association analysis of X-linked markers.
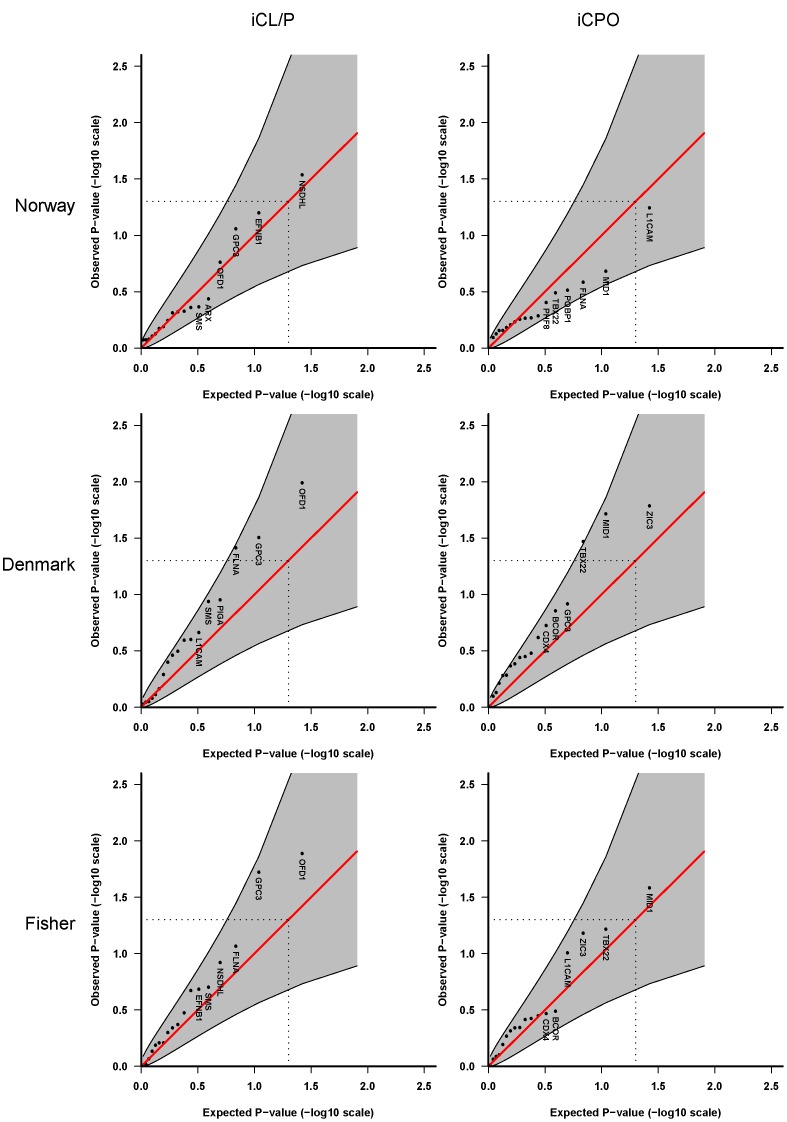
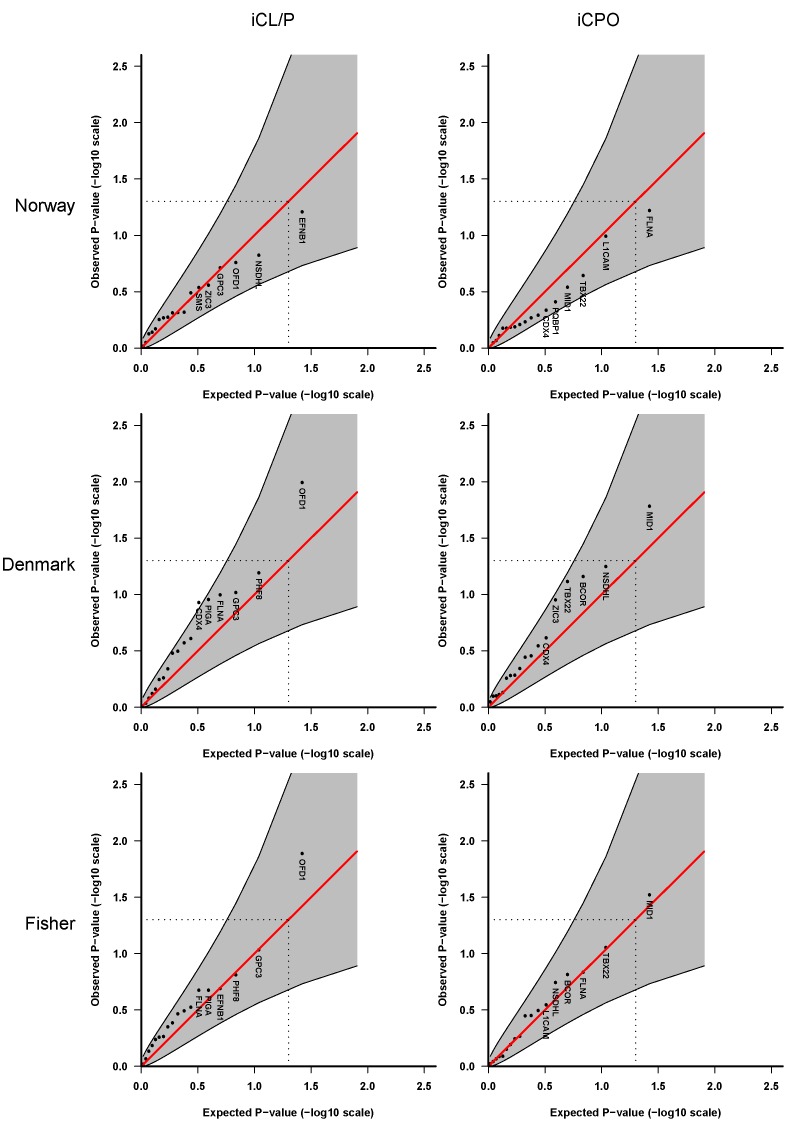
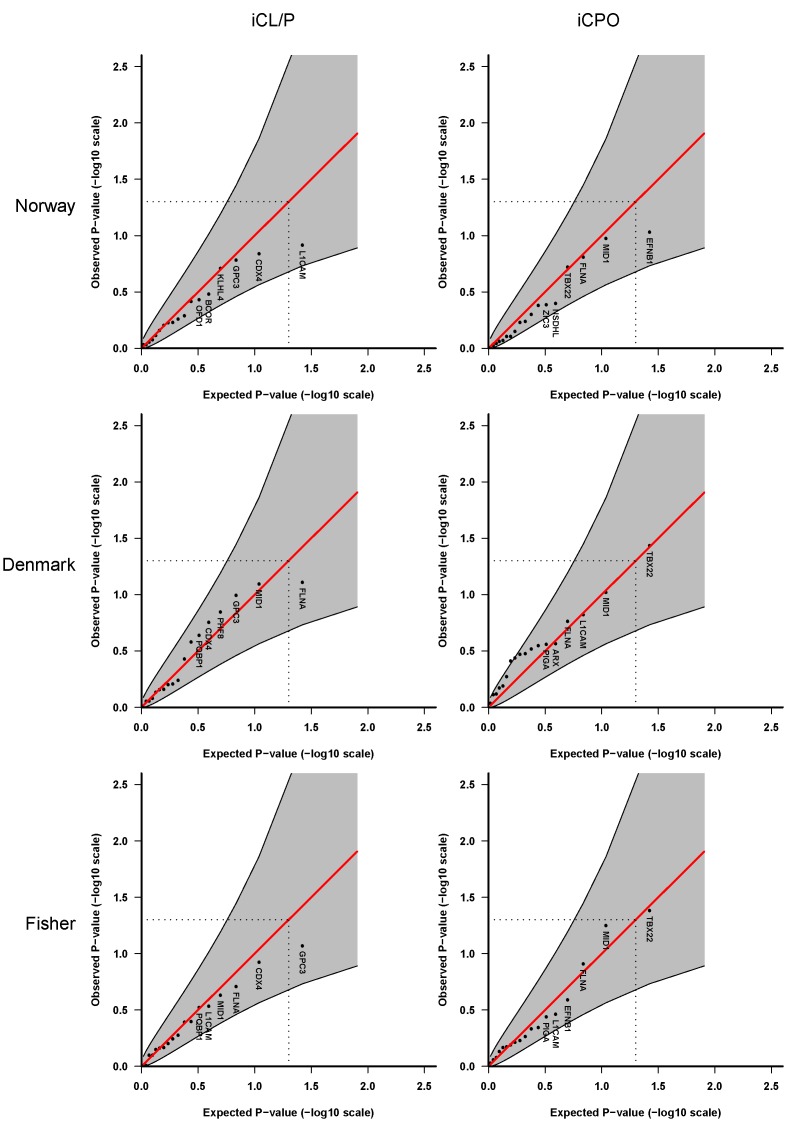
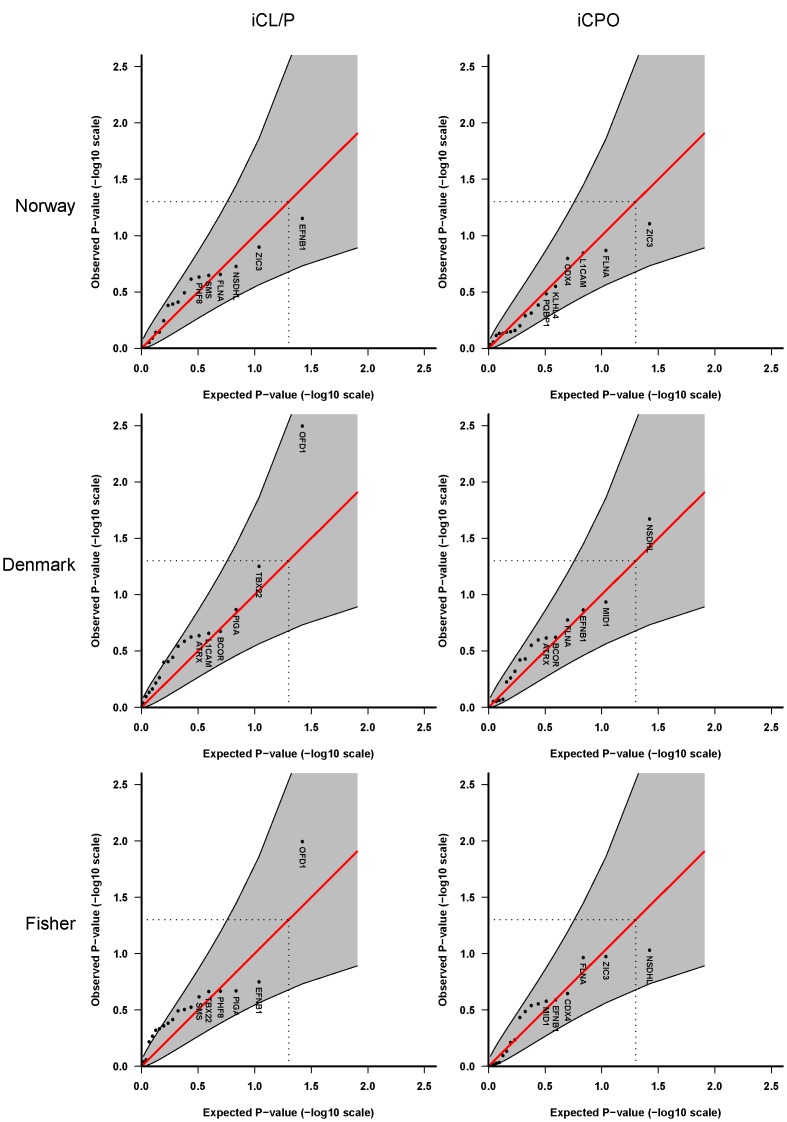
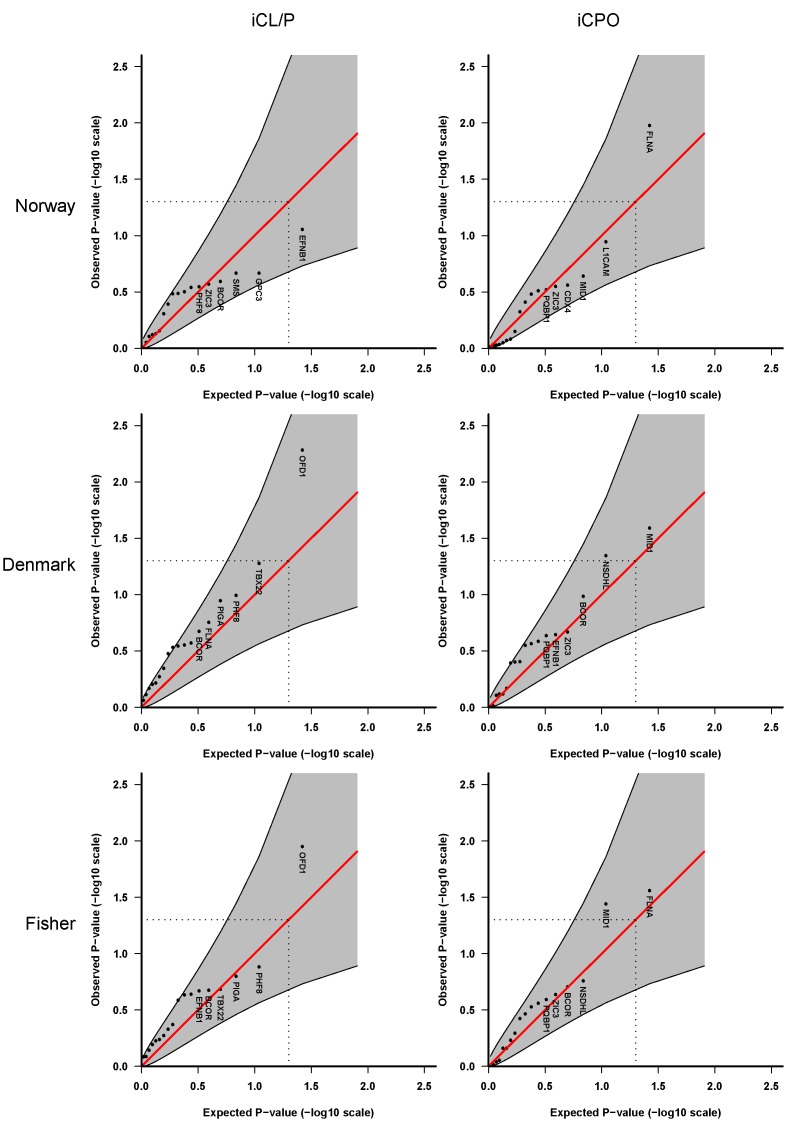
Methodology/principal findings: We added new functionalities in the HAPLIN statistical software to enable association analysis of X-linked markers and an exploration of various causal scenarios relevant to orofacial clefts. Genotypes for 48 SNPs in 18 candidate genes on the X chromosome were analyzed in two population-based samples from Scandinavia (562 Norwegian and 235 Danish case-parent triads). For haplotype analysis, we used a sliding-window approach and assessed isolated cleft lip with or without cleft palate (iCL/P) separately from isolated cleft palate only (iCPO). We tested three statistical models in HAPLIN, allowing for: i) the same relative risk in males and females, ii) sex-specific relative risks, and iii) X-inactivation in females. We found weak but consistent associations with the oral-facial-digital syndrome 1 (OFD1) gene (formerly known as CXORF5) in the Danish iCL/P samples across all models, but not in the Norwegian iCL/P samples. In sex-specific analyses, the association with OFD1 was in male cases only. No analyses showed associations with iCPO in either the Norwegian or the Danish sample.
Conclusions: The association of OFD1 with iCL/P is plausible given the biological relevance of this gene. However, the lack of replication in the Norwegian samples highlights the need to verify these preliminary findings in other large datasets. More generally, the novel analytic methods presented here are widely applicable to investigations of the role of X-linked genes in complex traits.
Conflict of interest statement
Figures
References
-
- Strauss RP. The organization and delivery of craniofacial health services: the state of the art. Cleft Palate Craniofac J. 1999;36:189–195. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
