

The Vermont Oxford Neonatal Encephalopathy Registry: rationale, methods, and initial results
- PMID: 22726296
- PMCID: PMC3502438
- DOI: 10.1186/1471-2431-12-84
The Vermont Oxford Neonatal Encephalopathy Registry: rationale, methods, and initial results
Abstract
Background: In 2006, the Vermont Oxford Network (VON) established the Neonatal Encephalopathy Registry (NER) to characterize infants born with neonatal encephalopathy, describe evaluations and medical treatments, monitor hypothermic therapy (HT) dissemination, define clinical research questions, and identify opportunities for improved care.
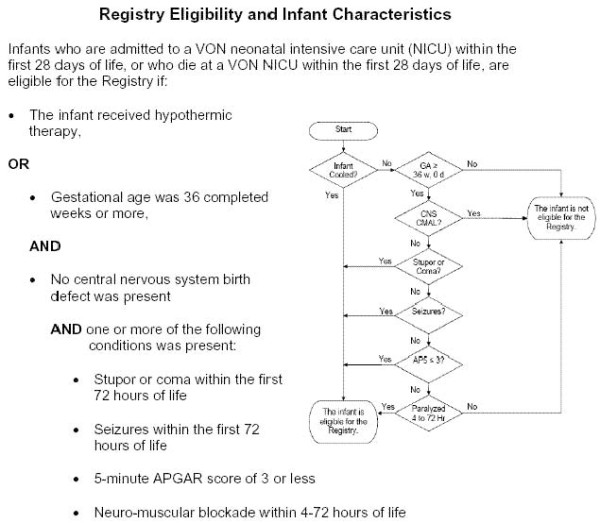
Methods: Eligible infants were ≥ 36 weeks with seizures, altered consciousness (stupor, coma) during the first 72 hours of life, a 5 minute Apgar score of ≤ 3, or receiving HT. Infants with central nervous system birth defects were excluded.
Results: From 2006-2010, 95 centers registered 4232 infants. Of those, 59% suffered a seizure, 50% had a 5 minute Apgar score of ≤ 3, 38% received HT, and 18% had stupor/coma documented on neurologic exam. Some infants experienced more than one eligibility criterion. Only 53% had a cord gas obtained and only 63% had a blood gas obtained within 24 hours of birth, important components for determining HT eligibility. Sixty-four percent received ventilator support, 65% received anticonvulsants, 66% had a head MRI, 23% had a cranial CT, 67% had a full channel encephalogram (EEG) and 33% amplitude integrated EEG. Of all infants, 87% survived.
Conclusions: The VON NER describes the heterogeneous population of infants with NE, the subset that received HT, their patterns of care, and outcomes. The optimal routine care of infants with neonatal encephalopathy is unknown. The registry method is well suited to identify opportunities for improvement in the care of infants affected by NE and study interventions such as HT as they are implemented in clinical practice.
Figures
References
-
- Nelson KB, Leviton A. How much of neonatal encephalopathy is due to birth asphyxia? Am J Dis Child. 1991;145(11):1325–1331. - PubMed
-
- Badawi N, Kurinczuk JJ, Keogh JM, Alessandri LM, O'Sullivan F, Burton PR, Pemberton PJ, Stanley FJ. Intrapartum risk factors for newborn encephalopathy: the Western Australian case–control study. BMJ Clinical research ed. 1998;317(7172):1554–1558. doi: 10.1136/bmj.317.7172.1554. - DOI - PMC - PubMed
-
- Levene MI, Sands C, Grindulis H, Moore JR. Comparison of two methods of predicting outcome in perinatal asphyxia. Lancet. 1986;1(8472):67–69. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
