

Socioeconomic inequality in the prevalence of noncommunicable diseases in low- and middle-income countries: results from the World Health Survey
- PMID: 22726343
- PMCID: PMC3490890
- DOI: 10.1186/1471-2458-12-474
Socioeconomic inequality in the prevalence of noncommunicable diseases in low- and middle-income countries: results from the World Health Survey
Abstract
Background: Noncommunicable diseases are an increasing health concern worldwide, but particularly in low- and middle-income countries. This study quantified and compared education- and wealth-based inequalities in the prevalence of five noncommunicable diseases (angina, arthritis, asthma, depression and diabetes) and comorbidity in low- and middle-income country groups.
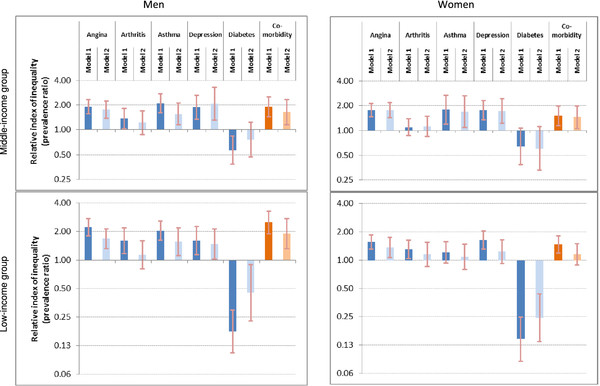
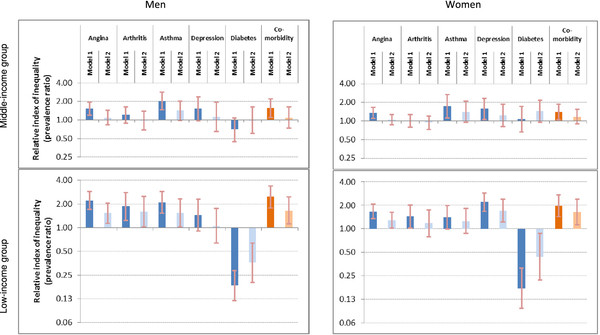
Methods: Using 2002-04 World Health Survey data from 41 low- and middle-income countries, the prevalence estimates of angina, arthritis, asthma, depression, diabetes and comorbidity in adults aged 18 years or above are presented for wealth quintiles and five education levels, by sex and country income group. Symptom-based classification was used to determine angina, arthritis, asthma and depression rates, and diabetes diagnoses were self-reported. Socioeconomic inequalities according to wealth and education were measured absolutely, using the slope index of inequality, and relatively, using the relative index of inequality.
Results: Wealth and education inequalities were more pronounced in the low-income country group than the middle-income country group. Both wealth and education were inversely associated with angina, arthritis, asthma, depression and comorbidity prevalence, with strongest inequalities reported for angina, asthma and comorbidity. Diabetes prevalence was positively associated with wealth and, to a lesser extent, education. Adjustments for confounding variables tended to decrease the magnitude of the inequality.
Conclusions: Noncommunicable diseases are not necessarily diseases of the wealthy, and showed unequal distribution across socioeconomic groups in low- and middle-income country groups. Disaggregated research is warranted to assess the impact of individual noncommunicable diseases according to socioeconomic indicators.
Figures
References
-
- World Health Organization. 2008–2013 action plan for the global strategy for the prevention and control of noncommunicable diseases: prevent and control cardiovascular diseases, cancers, chronic respiratory diseases and diabetes. World Health Organization, Geneva; 2008.
-
- World Health Organization. World Health Organization: Global status report on noncommunicable diseases. World Health Organization, Geneva; 2011.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
