

Severe and uncomplicated falciparum malaria in children from three regions and three ethnic groups in Cameroon: prospective study
- PMID: 22727184
- PMCID: PMC3445823
- DOI: 10.1186/1475-2875-11-215
Severe and uncomplicated falciparum malaria in children from three regions and three ethnic groups in Cameroon: prospective study
Abstract
Background: To identify the factors that account for differences in clinical outcomes of malaria as well as its relationship with ethnicity, transmission intensity and parasite density.
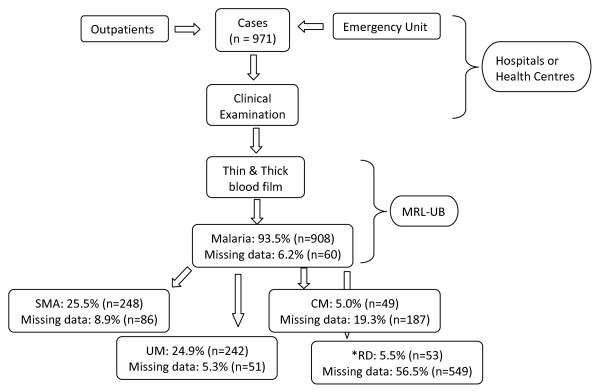
Methods: A prospective study was conducted in nine health facilities in the Centre, Littoral and South West regions of Cameroon, and in three ethnic groups; the Bantu, Semi-Bantu and Foulbe. Children aged one month to 13 years, with diagnosis suggestive of malaria, were recruited and characterized using the WHO definition for severe and uncomplicated malaria. Malaria parasitaemia was determined by light microscopy, haematological analysis using an automated haematology analyser and glucose level by colorimetric technique.
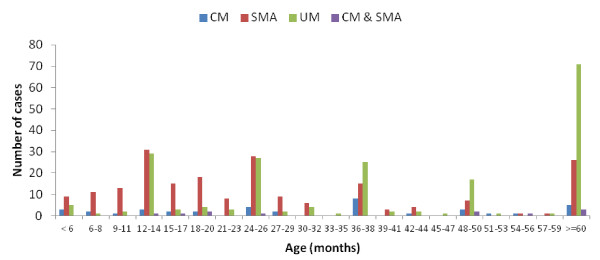
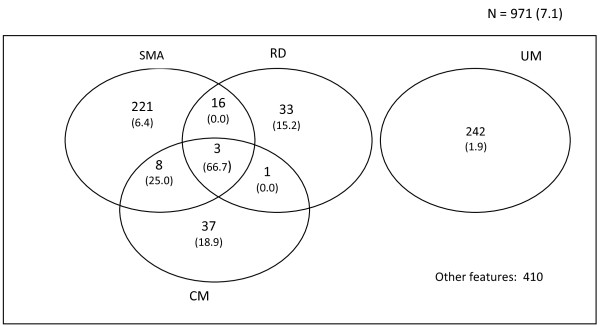
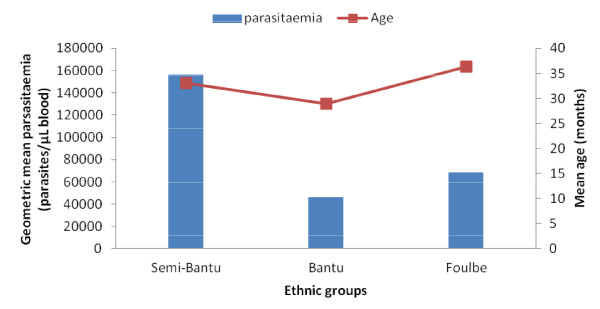
Results: Of the febrile children screened, 971 of the febrile children screened fulfilled the inclusion criteria for specific malaria clinical phenotypes. Forty-nine (9.2%) children had cerebral malaria, a feature that was similar across age groups, ethnicity and gender but lower (P < 0.004) in proportion in the Centre (3.1%, 5/163) compared to the Littoral (11.3%, 32/284) and South West (13.6%, 12/88) regions. Severe anaemia was the most frequent severe disease manifestation, 28.0% (248/885), which was similar in proportion across the three ethnic groups but was more prevalent in females, less than 60 months old, and the Centre region. About 20% (53/267) of the participants presented with respiratory distress, a clinical phenotype independent of age, gender and ethnicity, but highest (P < 0.001) in the Centre (55%, 11/20) compared to the Littoral (27.3%, 3/11) and South West (16.5%, 39/236) regions. Uncomplicated malaria constituted 27.7% (255/920) of hospital admissions and was similar in proportion with gender and across the three ethnic groups but more prevalent in older children (≥ 60 months) as well as in the South West region. The density of malaria parasitaemia was generally similar across clinical groups, gender and ethnicity. However, younger children and residents of the Centre region carried significantly higher parasite loads, with the burden heavier in the Semi-Bantu compared to their Bantu (P = 0.009) and Foulbe (P = 0.026) counterparts in the Centre region. The overall study case fatality was 4.8 (47/755), with cerebral malaria being the only significant risk factor associated with death. Severe anaemia, though a common and major clinical presentation, was not significantly associated with risk of death.
Conclusion: About half of the acutely febrile children presented with severe malaria, the majority being cases of severe malaria anaemia, followed by respiratory distress and cerebral malaria. The latter two were less prevalent in the Centre region compared to the other regions. Cerebral malaria and hyperpyrexia were the only significant risk factors associated with death.
Figures

References
-
- WHO. World Malaria report, Global malaria programme. World Health Organization Publication, Geneva; 2011.
-
- Malaney P, Speilman A, Sachs J. The malaria gap. Am J Trop Med Hyg. 2004;71:141–146. - PubMed
-
- Bremen JG. The ears of the hippopotamus: manifestations, determinants, and Estimates of the malaria burden. Am J Trop Med Hyg. 2001;64(Suppl 1–2):1–11. - PubMed
-
- Langhorne J, Ndungu FM, Sponaas A, Marsh K. Immunity to malaria: more questions than answers. Nat Immunol. 2008;9:725–732. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
