

Diagnosis and management of eosinophilic esophagitis
- PMID: 22728382
- PMCID: PMC3458791
- DOI: 10.1016/j.cgh.2012.06.003
Diagnosis and management of eosinophilic esophagitis
Abstract
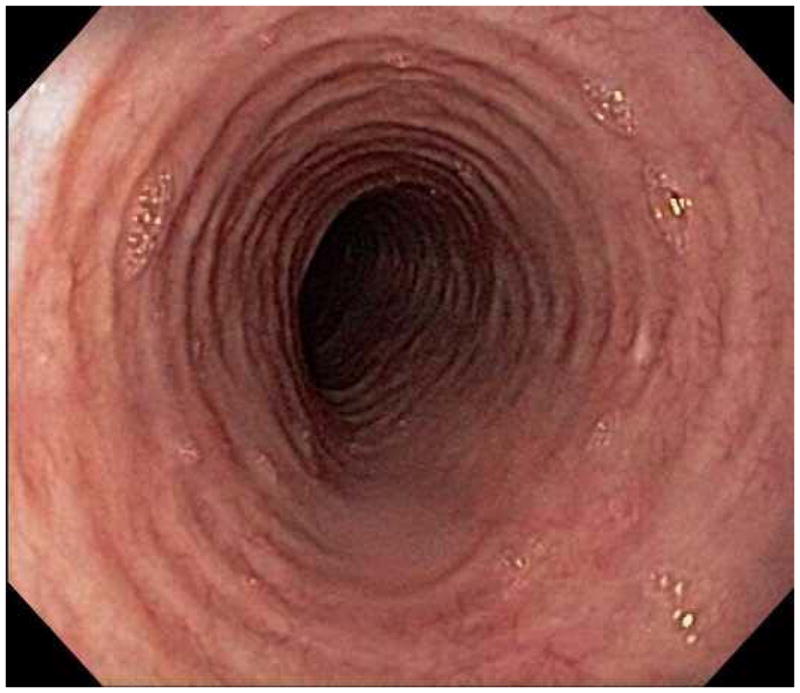
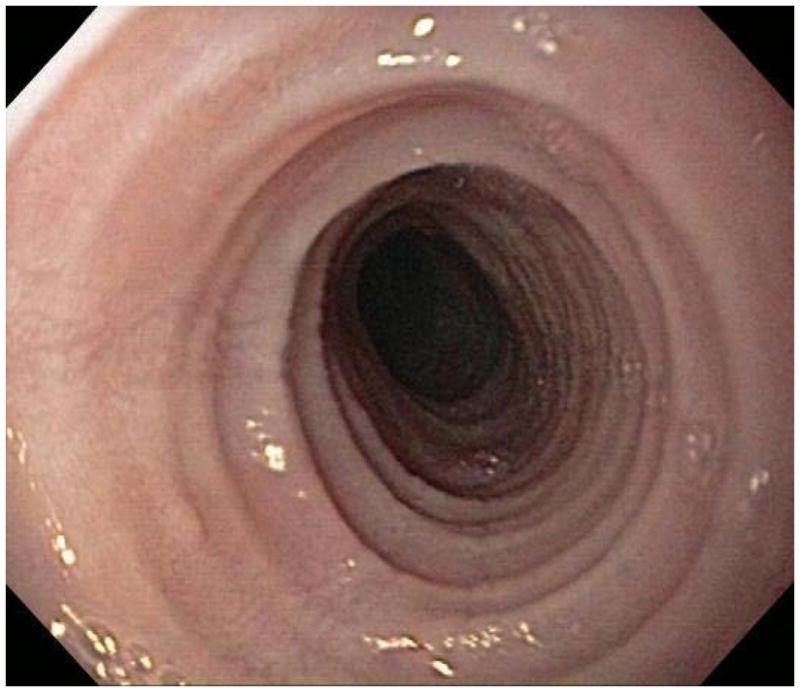
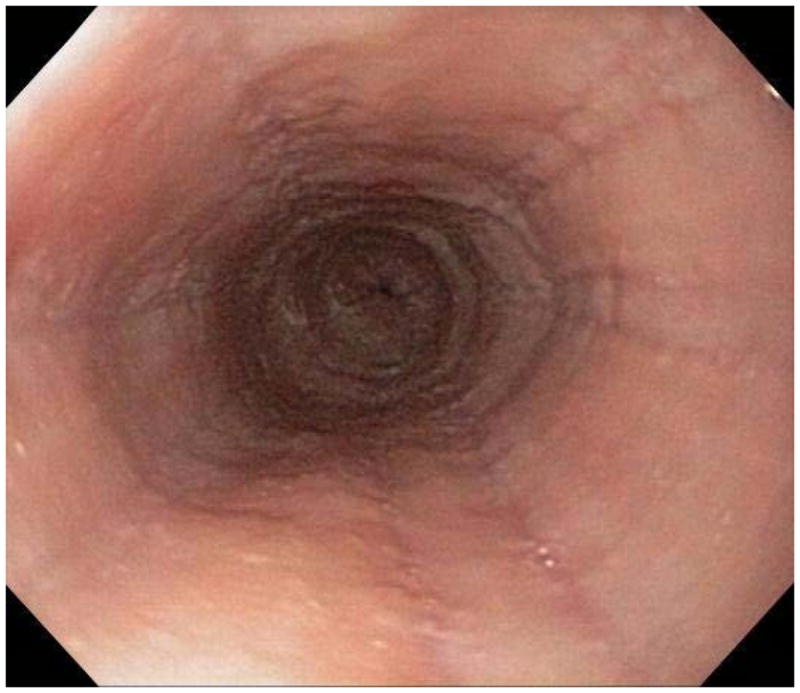
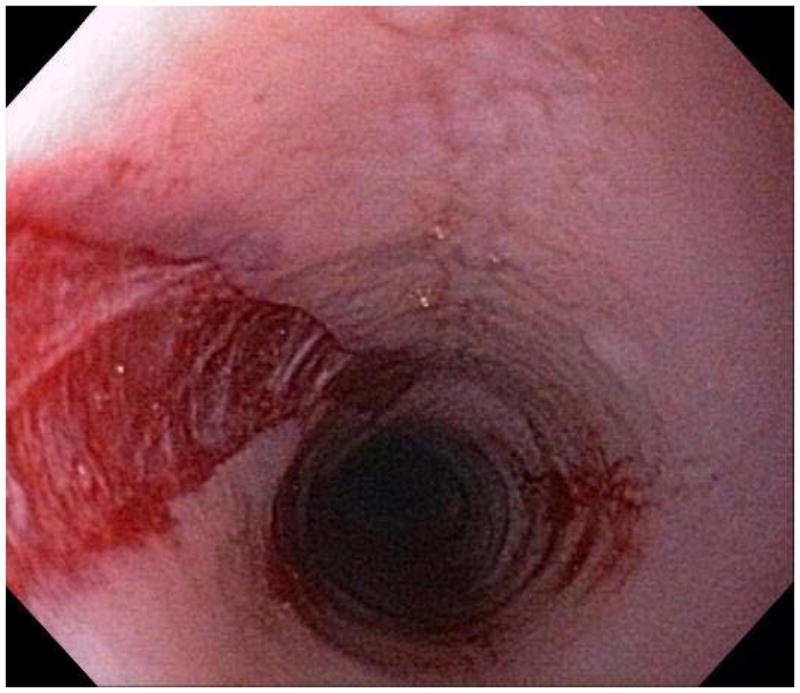
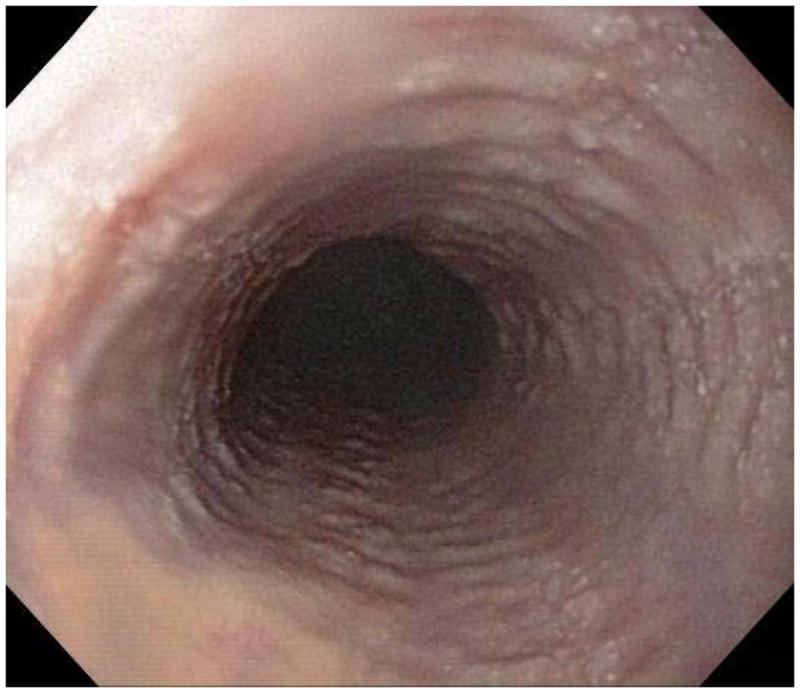
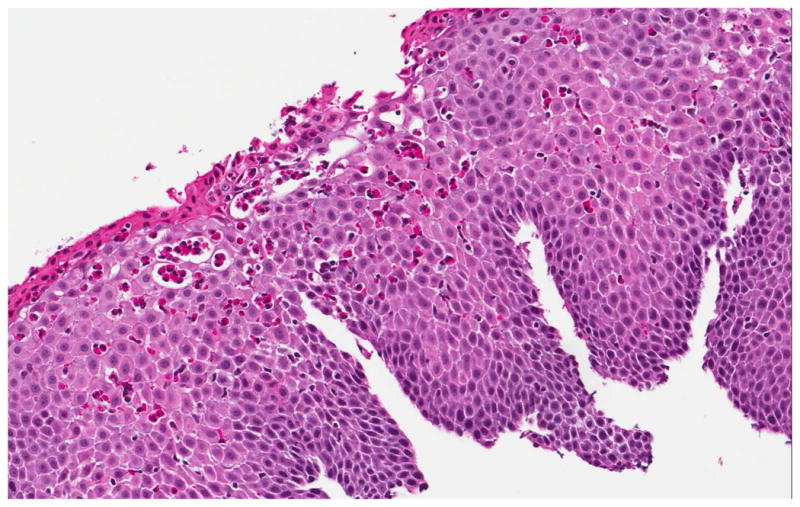
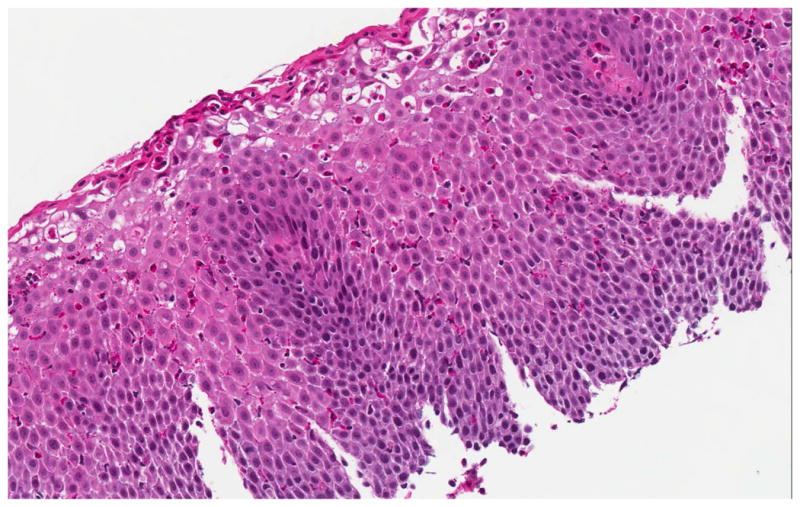
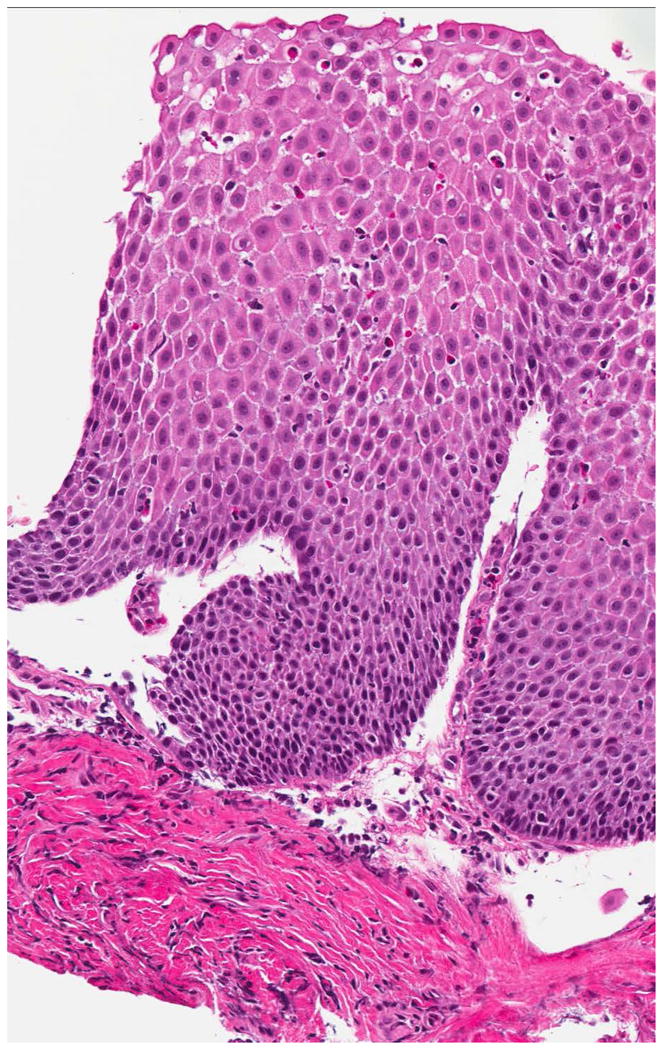
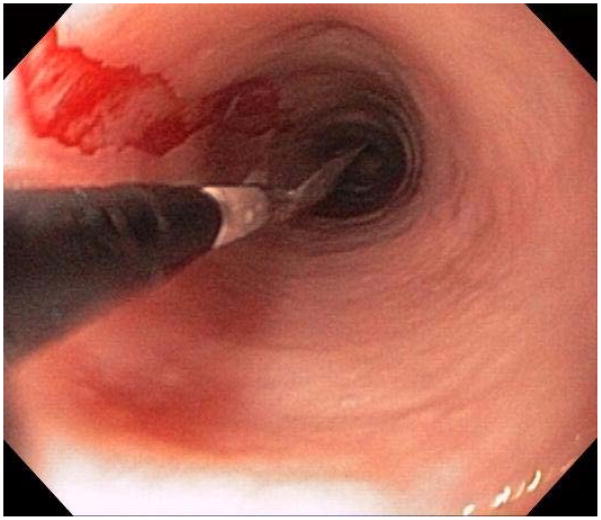
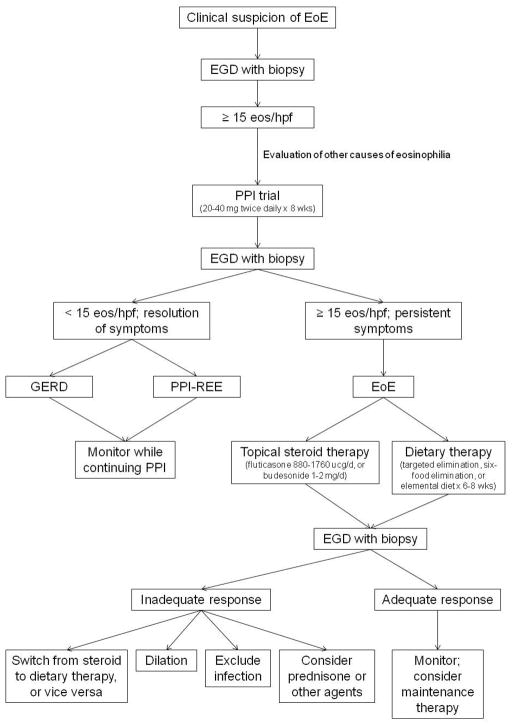
Eosinophilic esophagitis (EoE) is a chronic inflammatory condition characterized by esophageal dysfunction and eosinophilic infiltrate in the esophageal epithelium in the absence of other potential causes of eosinophilia. EoE is increasing in incidence and prevalence, and is a major cause of gastrointestinal morbidity among children and adults. EoE is thought to be immune mediated, with food or environmental antigens stimulating a T-helper (Th)-2 inflammatory response. An increased understanding of the pathogenesis of EoE has led to the evolution of diagnostic and treatment paradigms. We review the latest approach to diagnosis of EoE and present consensus diagnostic guidelines. We also discuss the clinical, endoscopic, and histologic features of EoE and challenges to diagnosis. Finally, we present the 3 major treatment options for EoE: pharmacologic therapy, dietary modification, and endoscopic dilation.
Copyright © 2012 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures: No conflicts of interested pertaining to this manuscript. Dr. Dellon has received research support from AstraZeneca, Meritage Pharma, Olympus, NIH, ACG, and AGA. Dr. Dellon has been a consultant for Oncoscope.
Figures


References
-
- Liacouras CA, Furuta GT, Hirano I, Atkins D, Attwood SE, Bonis PA, Burks AW, Chehade M, Collins MH, Dellon ES, Dohil R, Falk GW, Gonsalves N, Gupta SK, Katzka DA, Lucendo AJ, Markowitz JE, Noel RJ, Odze RD, Putnam PE, Richter JE, Romero Y, Ruchelli E, Sampson HA, Schoepfer A, Shaheen NJ, Sicherer SH, Spechler S, Spergel JM, Straumann A, Wershil BK, Rothenberg ME, Aceves SS. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011;128:3–20.e6. - PubMed
-
- Landres RT, Kuster GG, Strum WB. Eosinophilic esophagitis in a patient with vigorous achalasia. Gastroenterology. 1978;74:1298–1301. - PubMed
-
- Picus D, Frank PH. Eosinophilic esophagitis. AJR Am J Roentgenol. 1981;136:1001–3. - PubMed
-
- Lee RG. Marked eosinophilia in esophageal mucosal biopsies. Am J Surg Pathol. 1985;9:475–9. - PubMed
-
- Attwood SE, Smyrk TC, Demeester TR, Jones JB. Esophageal eosinophilia with dysphagia. A distinct clinicopathologic syndrome. Dig Dis Sci. 1993;38:109–16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
