

Predictive value of beat-to-beat QT variability index across the continuum of left ventricular dysfunction: competing risks of noncardiac or cardiovascular death and sudden or nonsudden cardiac death
- PMID: 22730411
- PMCID: PMC3432262
- DOI: 10.1161/CIRCEP.112.970541
Predictive value of beat-to-beat QT variability index across the continuum of left ventricular dysfunction: competing risks of noncardiac or cardiovascular death and sudden or nonsudden cardiac death
Abstract
Background: The goal of the present study was to determine the predictive value of beat-to-beat QT variability in heart failure patients across the continuum of left ventricular dysfunction.
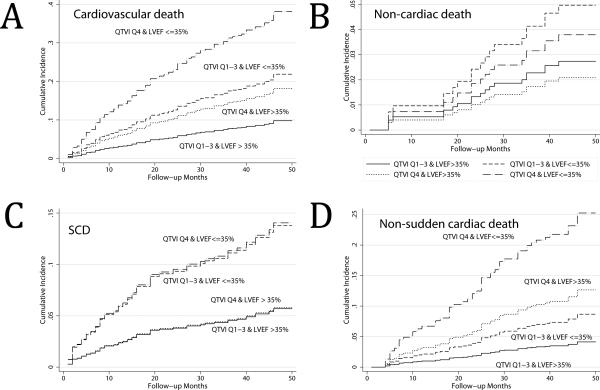
Methods and results: Beat-to-beat QT variability index (QTVI), log-transformed heart rate variance, normalized QT variance, and coherence between heart rate variability and QT variability have been measured at rest during sinus rhythm in 533 participants of the Muerte Subita en Insuficiencia Cardiaca heart failure study (mean age, 63.1±11.7; men, 70.6%; left ventricular ejection fraction >35% in 254 [48%]) and in 181 healthy participants from the Intercity Digital Electrocardiogram Alliance database. During a median of 3.7 years of follow-up, 116 patients died, 52 from sudden cardiac death (SCD). In multivariate competing risk analyses, the highest QTVI quartile was associated with cardiovascular death (subhazard ratio, 1.67 [95% CI, 1.14-2.47]; P=0.009) and, in particular, with non-SCD (subhazard ratio, 2.91 [1.69-5.01]; P<0.001). Elevated QTVI separated 97.5% of healthy individuals from subjects at risk for cardiovascular (subhazard ratio, 1.57 [1.04-2.35]; P=0.031) and non-SCD in multivariate competing risk model (subhazard ratio, 2.58 [1.13-3.78]; P=0.001). No interaction between QTVI and left ventricular ejection fraction was found. QTVI predicted neither noncardiac death (P=0.546) nor SCD (P=0.945). Decreased heart rate variability rather than increased QT variability was the reason for increased QTVI in the present study.
Conclusions: Increased QTVI because of depressed heart rate variability predicts cardiovascular mortality and non-SCD but neither SCD nor extracardiac mortality in heart failure across the continuum of left ventricular dysfunction. Abnormally augmented QTVI separates 97.5% of healthy individuals from heart failure patients at risk.
Figures



References
-
- Fang J, Mensah GA, Croft JB, Keenan NL. Heart failure-related hospitalization in the U.S., 1979 to 2004. J Am Coll Cardiol. 2008;52:428–434. - PubMed
-
- Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KK, Murabito JM, Vasan RS. Long-term trends in the incidence of and survival with heart failure. N. Engl. J Med. 2002;347:1397–1402. - PubMed
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De SG, Ferguson TB, Ford E, Furie K, Gillespie C, Go A, Greenlund K, Haase N, Hailpern S, Ho PM, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott MM, Meigs J, Mozaffarian D, Mussolino M, Nichol G, Roger VL, Rosamond W, Sacco R, Sorlie P, Roger VL, Thom T, Wasserthiel-Smoller S, Wong ND, Wylie-Rosett J. Heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010;121:e46–e215. - PubMed
-
- Liao L, Allen LA, Whellan DJ. Economic burden of heart failure in the elderly. Pharmacoeconomics. 2008;26:447–462. - PubMed
-
- The survival of patients with heart failure with preserved or reduced left ventricular ejection fraction: an individual patient data meta-analysis. European Heart Journal. 2011 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
