

Left ventricular twist is load-dependent as shown in a large animal model with controlled cardiac load
- PMID: 22731666
- PMCID: PMC3488500
- DOI: 10.1186/1476-7120-10-26
Left ventricular twist is load-dependent as shown in a large animal model with controlled cardiac load
Abstract
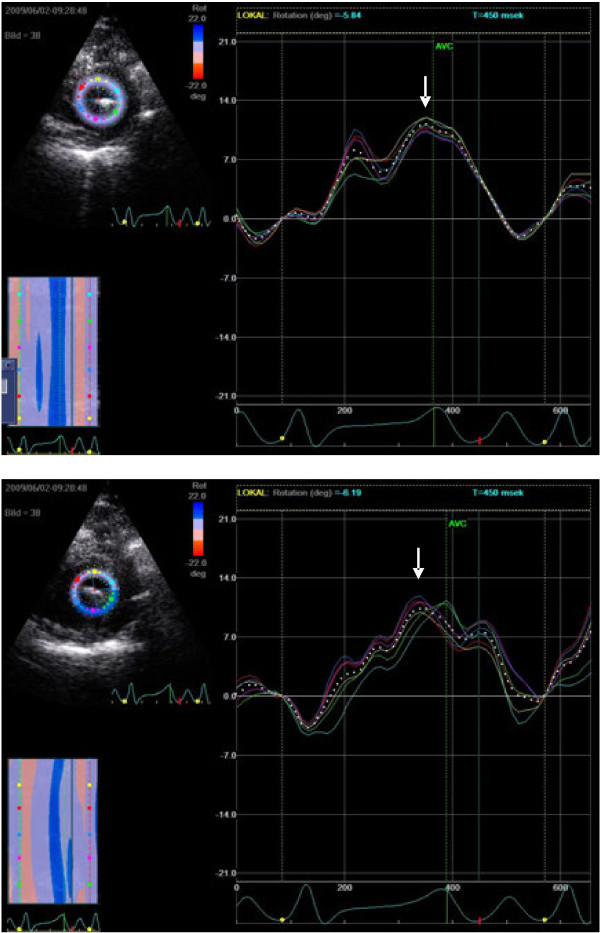
Background: Left ventricular rotation and twist can be assessed noninvasively by speckle tracking echocardiography. We sought to characterize the effects of acute load change and change in inotropic state on rotation parameters as a measure of left ventricular (LV) contractility.
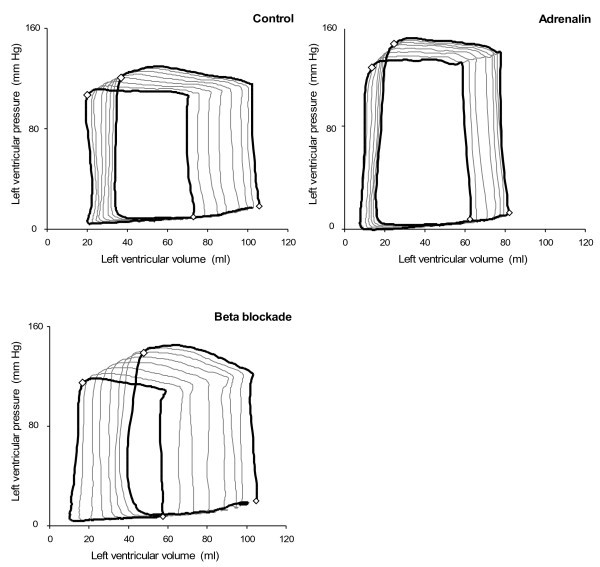
Methods: Seven anesthetised juvenile pigs were studied, using direct measurement of left ventricular pressure and volume and simultaneous transthoracic echocardiography. Transient inflation of an inferior vena cava balloon (IVCB) catheter produced controlled load reduction. First and last beats in the sequence of eight were analysed with speckle tracking (STE) during the load alteration and analysed for change in rotation/twist during controlled load alteration at same contractile status. Two pharmacological inotropic interventions were also included to examine the same hypothesis in additionally conditions of increased and decreased myocardial contractility in each animal. Paired comparisons were made for different load states using the Wilcoxon's Signed Rank test.
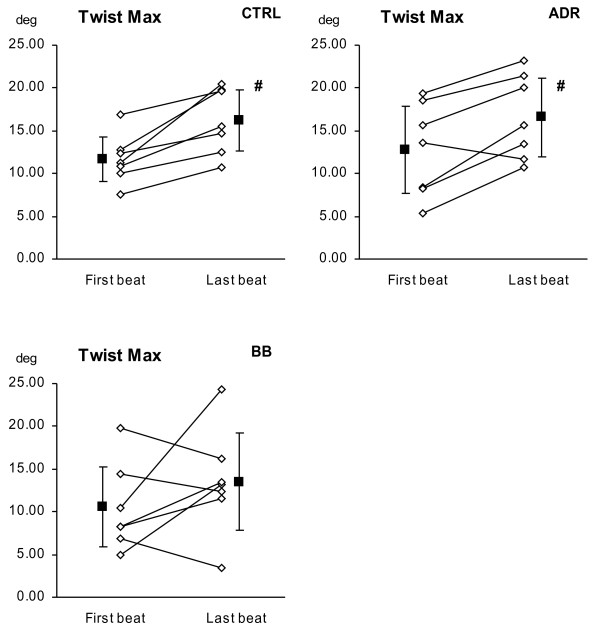
Results: The inferior vena cava balloon occlusion (IVCBO) load change compared for first to last beat resulted in LV twist increase (11.67° ±2.65° vs. 16.17° ±3.56° respectively, p < 0.004) during the load alteration and under adrenaline stimulation LV twist increase 12.56° ±5.1° vs. 16.57° ±4.6° (p < 0.013), and though increased, didn't reach significance in negative inotropic condition. Untwisting rate increased significantly at baseline from -41.7°/s ±41.6°/s vs.-122.6°/s ±55.8°/s (P < 0.039) and under adrenaline stimulation untwisting rate increased (-55.3°/s ±3.8°/s vs.-111.4°/s ±24.0°/s (p < 0.05), but did not systematically changed in negative inotropic condition.
Conclusions: Peak systolic LV twist and peak early diastolic untwisting rate are load dependent. Differences in LV load should be included in the interpretation when serial measures of twist are compared.
Figures
References
-
- Sengupta PP, Krishnamoorthy VK, Korinek J, Narula J, Vannan MA, Lester SJ, Tajik JA, Seward JB, Khandheria BK, Belohlavek M. Left ventricular form and function revisited: applied translational science to cardiovascular ultrasound imaging. J Am Soc Echocardiogr. 2007;20(5):539–551. doi: 10.1016/j.echo.2006.10.013. - DOI - PMC - PubMed
-
- Burns AT, La Gerche A, Prior DL, MacIsaac AI. Left ventricular untwisting is an important determinant of early diastolic function. J Am Coll Cardiol Img. 2009;2(6):709–716. - PubMed
-
- Sandstede JJ, Johnson T, Harre K, Beer M, Hofmann S, Pabst T, Kenn W, Voelker W, Neubauer S, Hahn D. Cardiac systolic rotation and contraction before and after valve replacement for aortic stenosis: a myocardial tagging study using MR imaging. AJR Am J Roentgenol. 2002;178(4):953–958. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
