

Costs and infant outcomes after implementation of a care process model for febrile infants
- PMID: 22732178
- PMCID: PMC4074609
- DOI: 10.1542/peds.2012-0127
Costs and infant outcomes after implementation of a care process model for febrile infants
Abstract
Objective: Febrile infants in the first 90 days may have life-threatening serious bacterial infection (SBI). Well-appearing febrile infants with SBI cannot be distinguished from those without by examination alone. Variation in care resulting in both undertreatment and overtreatment is common.
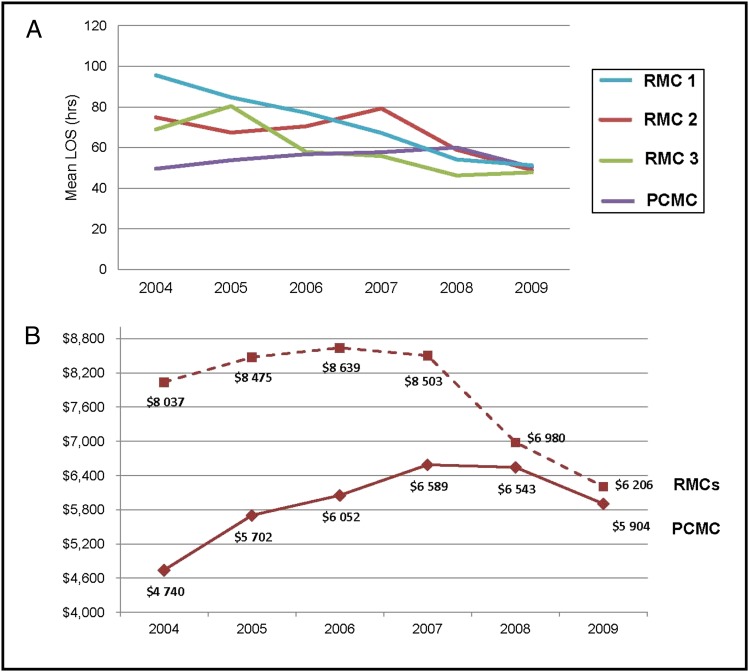
Methods: We developed and implemented an evidence-based care process model (EB-CPM) for the management of well-appearing febrile infants in the Intermountain Healthcare System. We report an observational study describing changes in (1) care delivery, (2) outcomes of febrile infants, and (3) costs before and after implementation of the EB-CPM in a children's hospital and in regional medical centers.
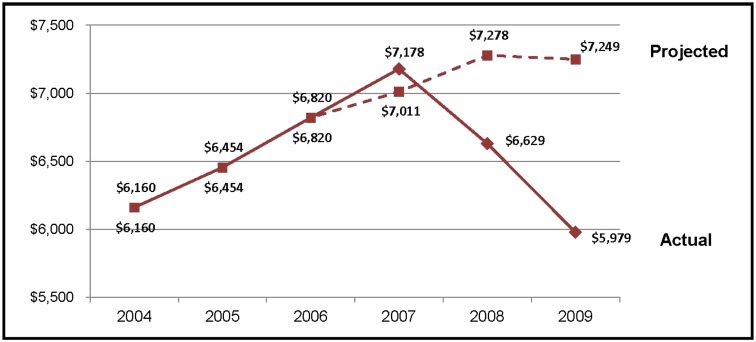
Results: From 2004 through 2009, 8044 infants had 8431 febrile episodes, resulting in medical evaluation. After implementation of the EB-CPM in 2008, infants in all facilities were more likely to receive evidence-based care including appropriate diagnostic testing, determination of risk for SBI, antibiotic selection, decreased antibiotic duration, and shorter hospital stays (P < .001 for all). In addition, more infants had a definitive diagnosis of urinary tract infection or viral illness (P < .001 for both). Infant outcomes improved with more admitted infants positive for SBI (P = .011), and infants at low risk for SBI were more often managed without antibiotics (P < .001). Although hospital admissions were shortened by 27%, there were no cases of missed SBI. Health Care costs were also reduced, with the mean cost per admitted infant decreasing from $7178 in 2007 to $5979 in 2009 (-17%, P < .001).
Conclusions: The EB-CPM increased evidence-based care in all facilities. Infant outcomes improved and costs were reduced, substantially improving value.
Figures
Comment in
-
Febrile infants: aligning science, guidelines, and cost reduction with quality of individualized care.Pediatrics. 2012 Jul;130(1):e199-200. doi: 10.1542/peds.2012-1178. Epub 2012 Jun 25. Pediatrics. 2012. PMID: 22732175 No abstract available.
References
-
- Byington CL, Enriquez FR, Hoff C, et al. . Serious bacterial infections in febrile infants 1 to 90 days old with and without viral infections. Pediatrics. 2004;113(6):1662–1666 - PubMed
-
- Baraff LJ, Oslund SA, Schriger DL, Stephen ML. Probability of bacterial infections in febrile infants less than three months of age: a meta-analysis. Pediatr Infect Dis J. 1992;11(4):257–264 - PubMed
-
- Greenes DS, Harper MB. Low risk of bacteremia in febrile children with recognizable viral syndromes. Pediatr Infect Dis J. 1999;18(3):258–261 - PubMed
-
- Bender JM, Ampofo K, Gesteland P, et al. . Influenza virus infection in infants less than three months of age. Pediatr Infect Dis J. 2010;29(1):6–9 - PubMed
-
- Rittichier KR, Bryan PA, Bassett KE, et al. . Diagnosis and outcomes of enterovirus infections in young infants. Pediatr Infect Dis J. 2005;24(6):546–550 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
