

High levels of circulating epinephrine trigger apical cardiodepression in a β2-adrenergic receptor/Gi-dependent manner: a new model of Takotsubo cardiomyopathy
- PMID: 22732314
- PMCID: PMC4890655
- DOI: 10.1161/CIRCULATIONAHA.112.111591
High levels of circulating epinephrine trigger apical cardiodepression in a β2-adrenergic receptor/Gi-dependent manner: a new model of Takotsubo cardiomyopathy
Abstract
Background: Takotsubo cardiomyopathy is an acute heart failure syndrome characterized by myocardial hypocontractility from the mid left ventricle to the apex. It is precipitated by extreme stress and can be triggered by intravenous catecholamine administration, particularly epinephrine. Despite its grave presentation, Takotsubo cardiomyopathy is rapidly reversible, with generally good prognosis. We hypothesized that this represents switching of epinephrine signaling through the pleiotropic β(2)-adrenergic receptor (β(2)AR) from canonical stimulatory G-protein-activated cardiostimulant to inhibitory G-protein-activated cardiodepressant pathways.
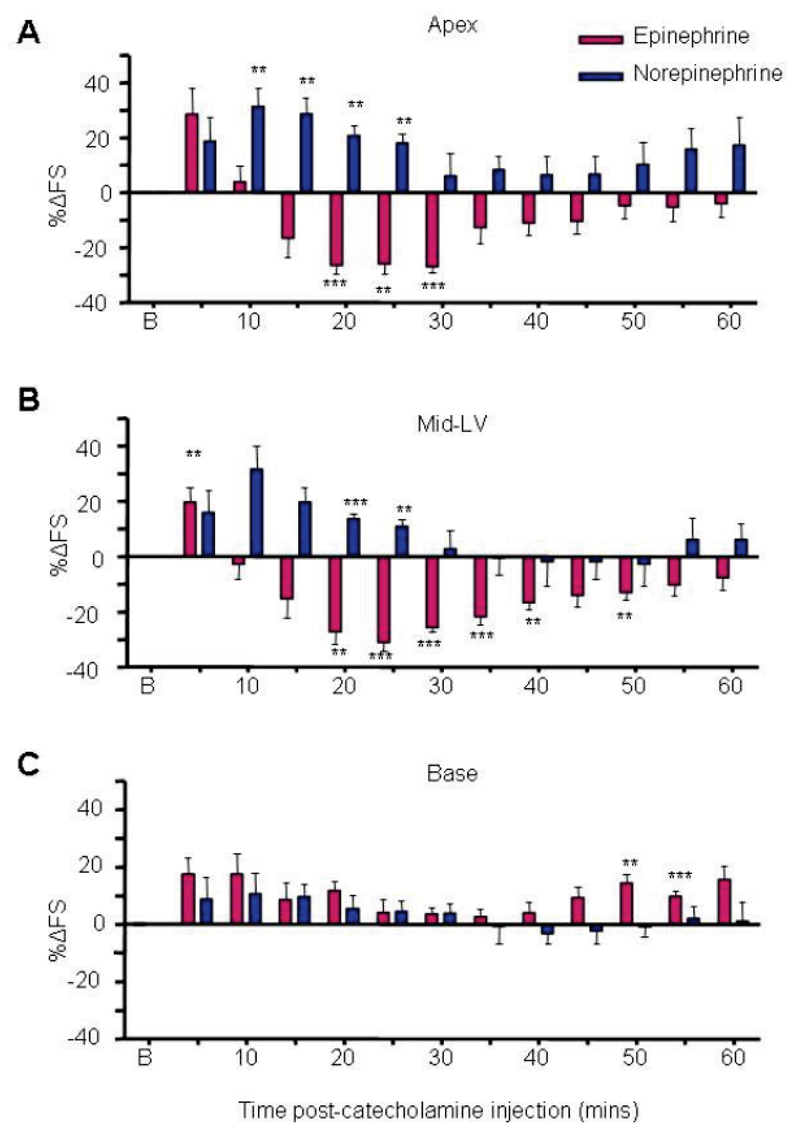
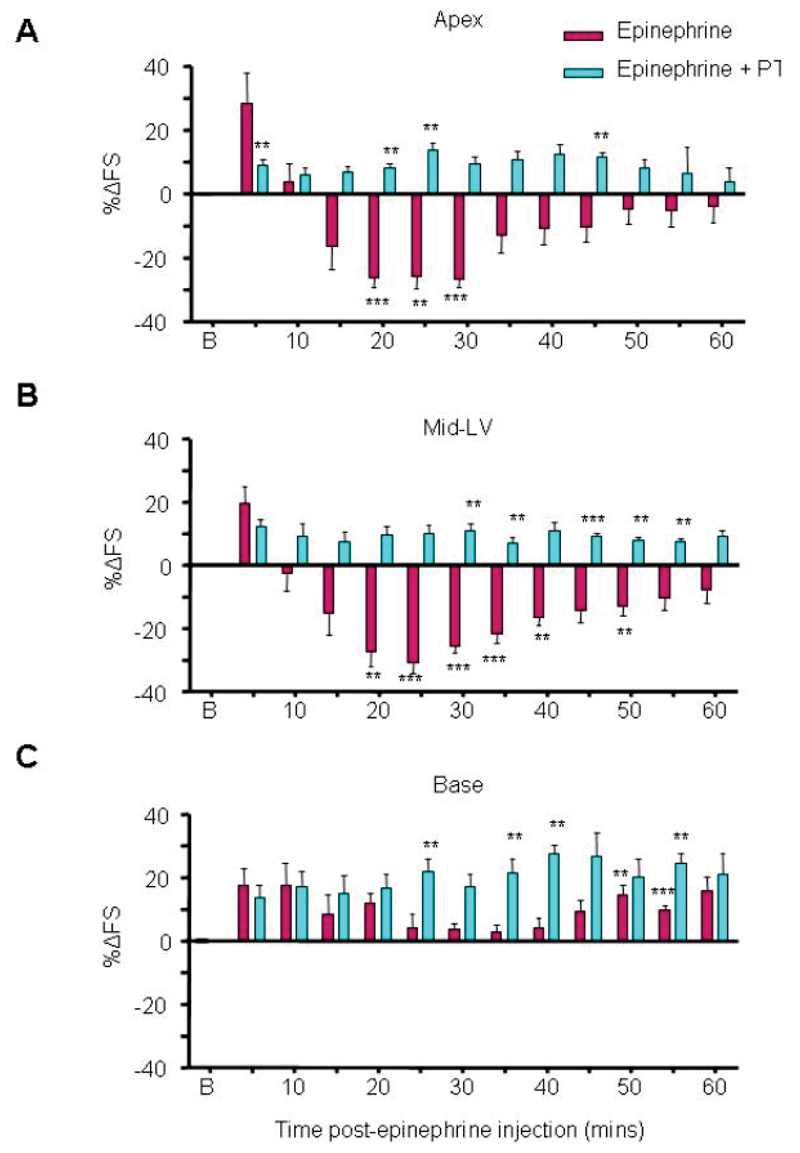
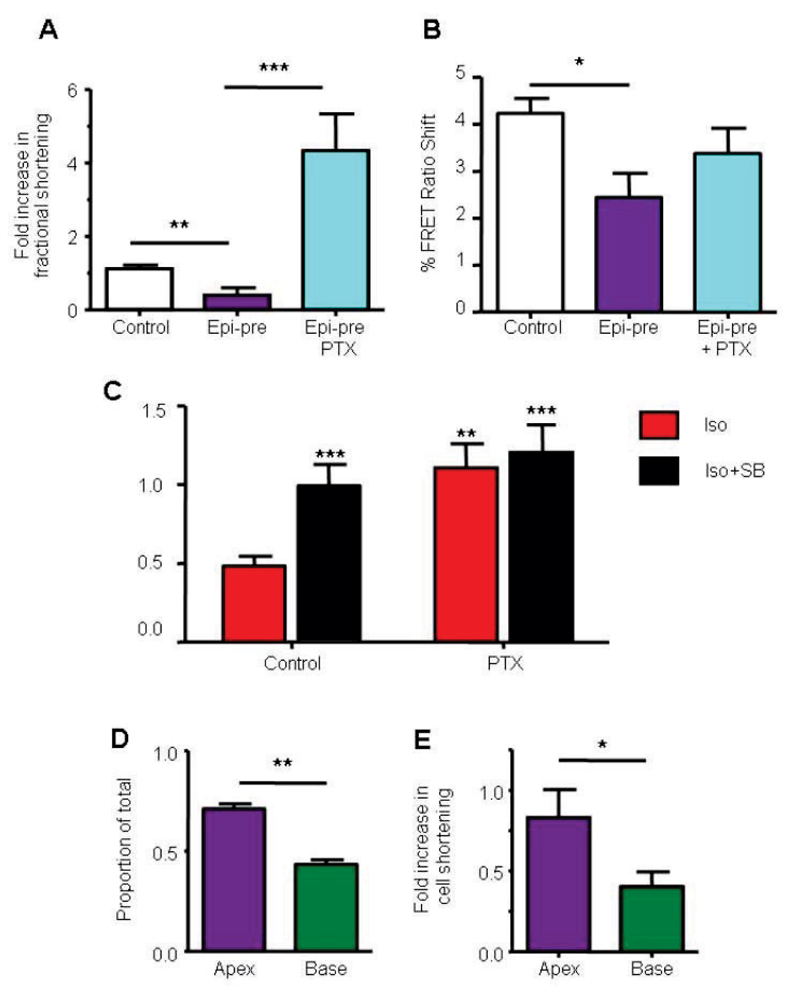
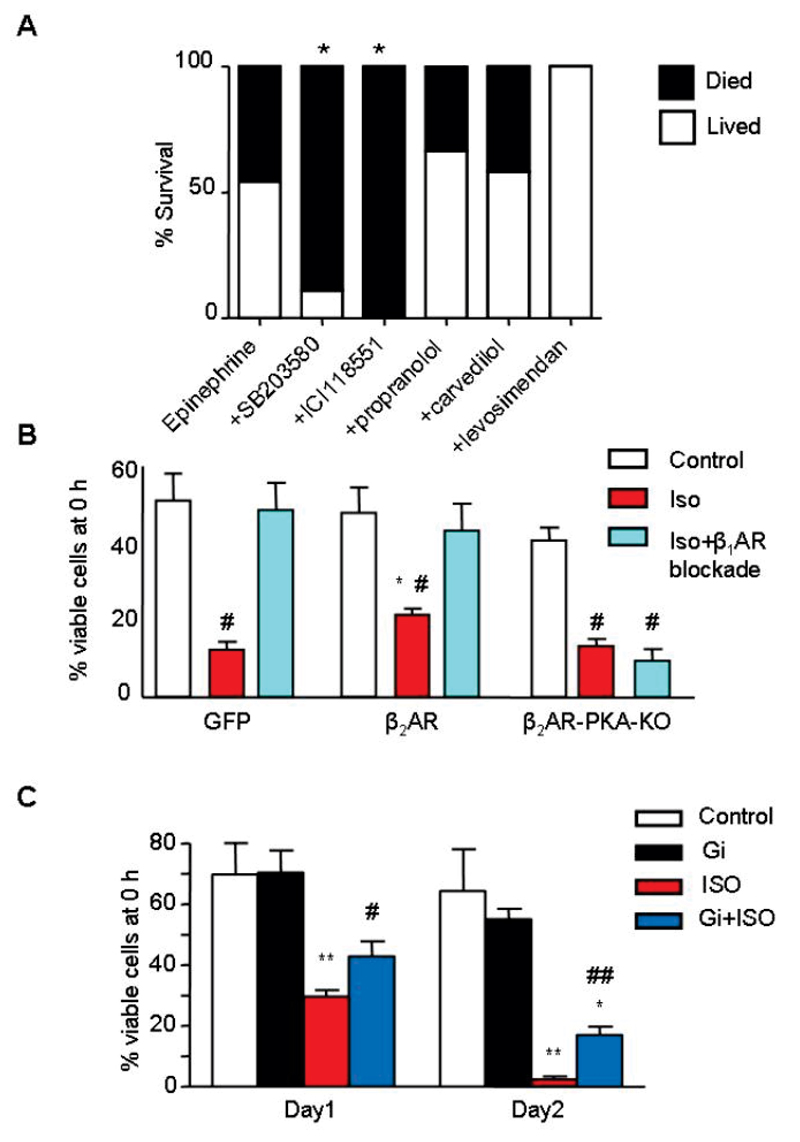
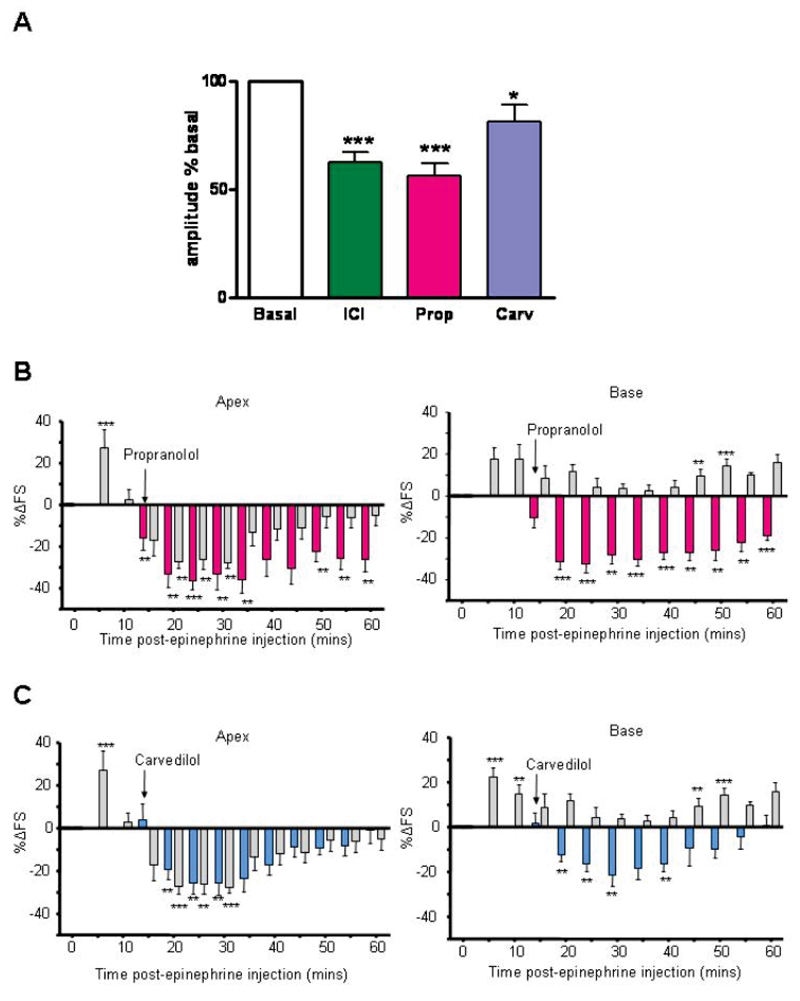
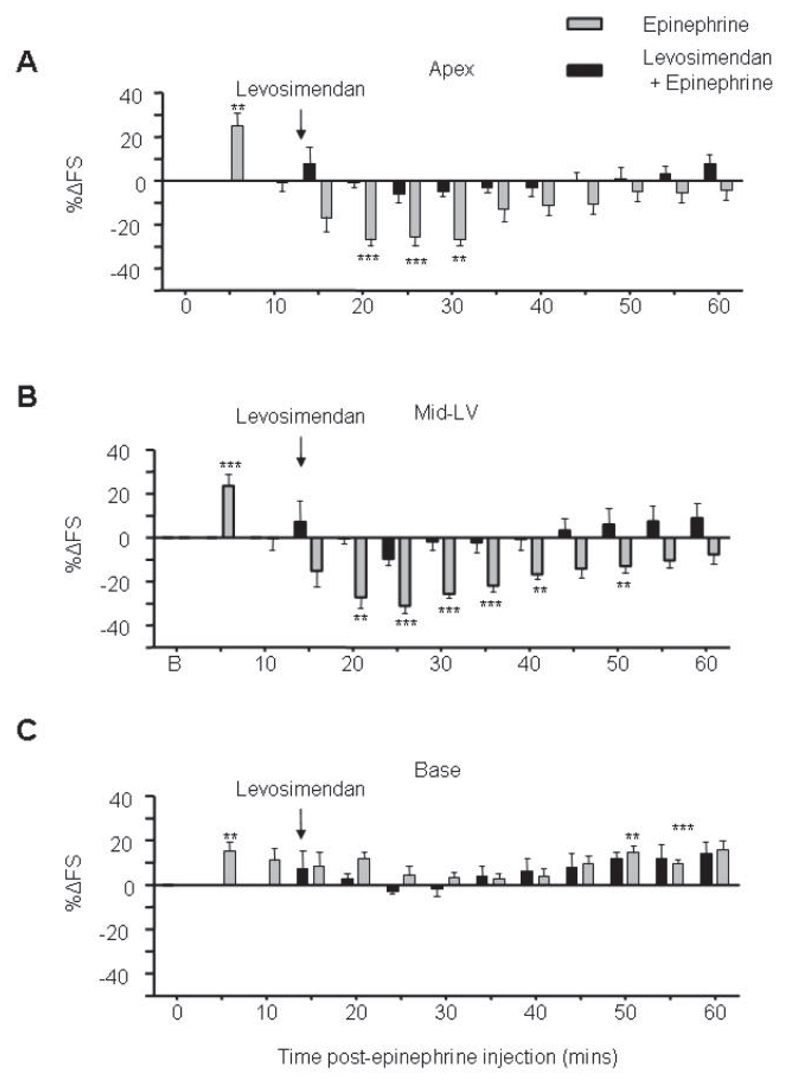
Methods and results: We describe an in vivo rat model in which a high intravenous epinephrine, but not norepinephrine, bolus produces the characteristic reversible apical depression of myocardial contraction coupled with basal hypercontractility. The effect is prevented via G(i) inactivation by pertussis toxin pretreatment. β(2)AR number and functional responses were greater in isolated apical cardiomyocytes than in basal cardiomyocytes, which confirmed the higher apical sensitivity and response to circulating epinephrine. In vitro studies demonstrated high-dose epinephrine can induce direct cardiomyocyte cardiodepression and cardioprotection in a β(2)AR-Gi-dependent manner. Preventing epinephrine-G(i) effects increased mortality in the Takotsubo model, whereas β-blockers that activate β(2)AR-G(i) exacerbated the epinephrine-dependent negative inotropic effects without further deaths. In contrast, levosimendan rescued the acute cardiac dysfunction without increased mortality.
Conclusions: We suggest that biased agonism of epinephrine for β(2)AR-G(s) at low concentrations and for G(i) at high concentrations underpins the acute apical cardiodepression observed in Takotsubo cardiomyopathy, with an apical-basal gradient in β(2)ARs explaining the differential regional responses. We suggest this epinephrine-specific β(2)AR-G(i) signaling may have evolved as a cardioprotective strategy to limit catecholamine-induced myocardial toxicity during acute stress.
Conflict of interest statement
Figures
References
-
- Wittstein IS, Thiemann DR, Lima JAC, Baughman KL, Schulman SP, Gerstenblith G, Wu KC, Rade JJ, Bivalacqua TJ, Champion HC. Neurohumoral Features of Myocardial Stunning Due to Sudden Emotional Stress. N Engl J Med. 2005;352:539–548. - PubMed
-
- Prasad A. Apical Ballooning Syndrome: An Important Differential Diagnosis of Acute Myocardial Infarction. Circulation. 2007;115:56–59. - PubMed
-
- Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006;27:1523–1529. - PubMed
-
- Sato M, Fujita S, Saito A, Ikeda Y, Kitazawa H, Takahashi M, Ishiguro J, Okabe M, Nakamura Y, Nagai T, Watanabe H, et al. Increased incidence of transient left ventricular apical ballooning (so-called 'Takotsubo' cardiomyopathy) after the mid-Niigata Prefecture earthquake. Circ J. 2006;70:947–953. - PubMed
-
- Lenders JW, Eisenhofer G, Mannelli M, Pacak K. Phaeochromocytoma. Lancet. 2005;366:665–675. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
