

Pelvic tilt and trunk inclination: new predictive factors in curve progression during the Milwaukee bracing for adolescent idiopathic scoliosis
- PMID: 22732829
- PMCID: PMC3463696
- DOI: 10.1007/s00586-012-2409-6
Pelvic tilt and trunk inclination: new predictive factors in curve progression during the Milwaukee bracing for adolescent idiopathic scoliosis
Abstract
Introduction: Previous studies had shown that sagittal spinal and pelvic morphology may be associated with the development and progression of adolescent idiopathic scoliosis, but the predictive value of initial spinal and pelvic morphology on the curve progression during brace treatment is unknown. The objective of this study was to evaluate the relation between initial spinopelvic morphology and the risk of curve progression of adolescent idiopathic scoliosis with the Milwaukee brace.
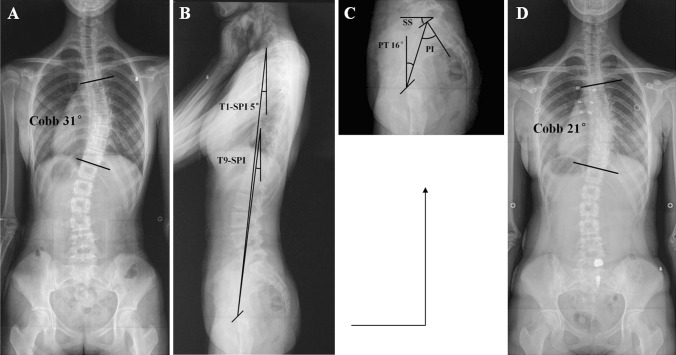
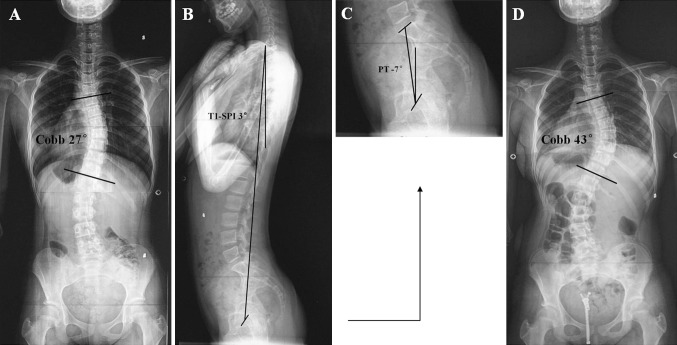
Materials and methods: From 2002 to 2007, adolescent idiopathic scoliosis (single thoracic curve with apex at or above T8) was treated with the Milwaukee brace in 60 girls. Initial standing, full-length lateral radiographs were made and seven sagittal radiographic parameters of spinal and pelvic alignment were measured. Patients were followed until skeletal maturity or progression of Cobb angle >45°. The progression of curve was defined as an increase of Cobb angle ≥6° at final follow-up or progression to surgery during brace treatment.
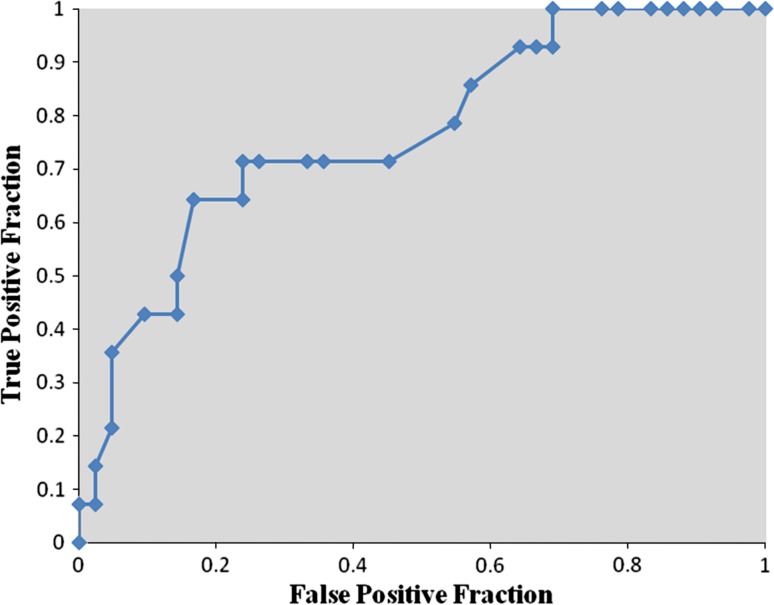
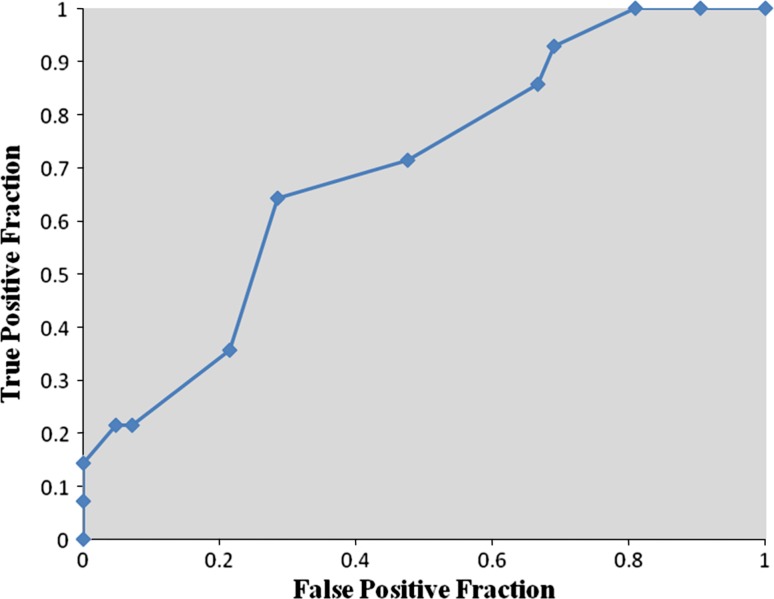
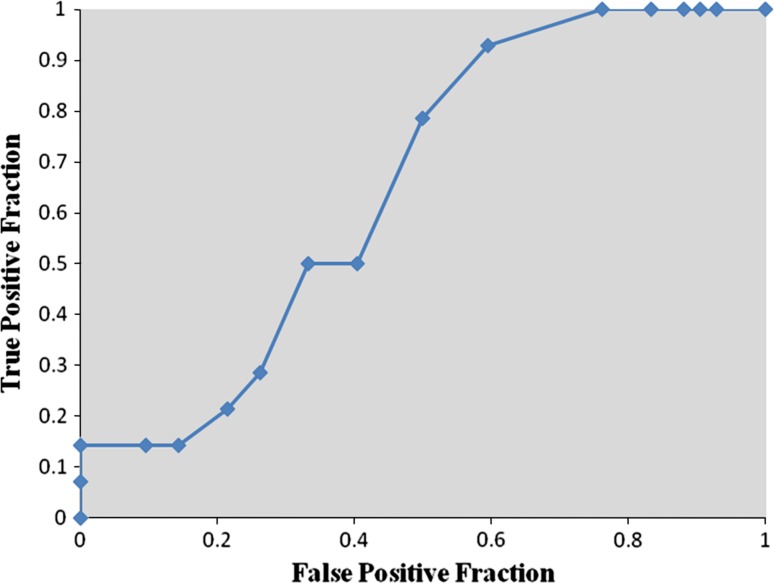
Results: The 45 patients (75.0 %) who had successful control of curve progression were initially significantly more skeletally mature (higher mean Risser sign) than the 15 patients (25.0 %) who had curve progression. The initial mean Cobb angle was similar between the stable and progressed groups. The mean pelvic tilt, T1-spinopelvic inclination and T9-spinopelvic inclination angles were significantly greater in the stable group than in the progressed group and these three angles were independent predictors for curve progression during brace treatment. There were no significant differences between the stable and progressed groups in initial mean pelvic incidence, sacral slope, thoracic kyphosis or lumbar lordosis angles. Pre-bracing pelvic tilt ≤-0.5° was strongly predictive and T1-spinopelvic inclination ≤3.5° was moderately predictive of curve progression during the Milwaukee brace treatment.
Conclusions: Initial pelvic tilt and spinopelvic inclination angles may predict the curve progression and treatment outcome of adolescent idiopathic scoliosis with the Milwaukee brace.
Figures
Similar articles
-
Staying ahead of the curve: the use of spinopelvic parameters to predict curve progression and bracing success in adolescent idiopathic scoliosis.Spine Deform. 2020 Dec;8(6):1213-1222. doi: 10.1007/s43390-020-00159-5. Epub 2020 Jul 21. Spine Deform. 2020. PMID: 32696447
-
Differences in early sagittal plane alignment between thoracic and lumbar adolescent idiopathic scoliosis.Spine J. 2014 Feb 1;14(2):282-90. doi: 10.1016/j.spinee.2013.08.059. Epub 2013 Nov 12. Spine J. 2014. PMID: 24231781 Clinical Trial.
-
Nighttime bracing with the Providence brace in adolescent girls with idiopathic scoliosis.Spine (Phila Pa 1976). 2001 Sep 15;26(18):2006-12. doi: 10.1097/00007632-200109150-00014. Spine (Phila Pa 1976). 2001. PMID: 11547201
-
Discontinuation of brace treatment in adolescent idiopathic scoliosis (AIS): a scoping review.Spine Deform. 2024 Sep;12(5):1217-1228. doi: 10.1007/s43390-024-00882-3. Epub 2024 May 1. Spine Deform. 2024. PMID: 38693334 Free PMC article.
-
Curve type, flexibility, correction, and rotation are predictors of curve progression in patients with adolescent idiopathic scoliosis undergoing conservative treatment : a systematic review.Bone Joint J. 2022 Apr;104-B(4):424-432. doi: 10.1302/0301-620X.104B4.BJJ-2021-1677.R1. Bone Joint J. 2022. PMID: 35360948 Free PMC article.
Cited by
-
Factors relating to curve progression in female patients with adolescent idiopathic scoliosis treated with a brace.Eur Spine J. 2015 Feb;24(2):244-8. doi: 10.1007/s00586-014-3674-3. Epub 2014 Nov 26. Eur Spine J. 2015. PMID: 25424687
-
Digital study and correlation analysis of sagittal balance parameters in adolescents with idiopathic scoliosis: A comparative study with healthy adolescents.PLoS One. 2025 Jun 18;20(6):e0326233. doi: 10.1371/journal.pone.0326233. eCollection 2025. PLoS One. 2025. PMID: 40531946 Free PMC article.
-
Accuracy of intraoperative approximation of pelvic tilt using preoperative standing radiographs.J Orthop. 2024 Mar 22;54:120-123. doi: 10.1016/j.jor.2024.03.026. eCollection 2024 Aug. J Orthop. 2024. PMID: 38560587 Free PMC article.
-
High-heeled-related alterations in the static sagittal profile of the spino-pelvic structure in young women.Eur Spine J. 2015 Jun;24(6):1274-81. doi: 10.1007/s00586-015-3857-6. Epub 2015 Mar 10. Eur Spine J. 2015. PMID: 25753007
-
Rib-vertebral angle measurements predict brace treatment outcome in Risser grade 0 and premenarchal girls with adolescent idiopathic scoliosis.Eur Spine J. 2016 Oct;25(10):3088-3094. doi: 10.1007/s00586-015-4372-5. Epub 2016 Jan 23. Eur Spine J. 2016. PMID: 26803296
References
-
- Carr WA, Moe JH, Winter RB, Lonstein JE. Treatment of idiopathic scoliosis in the Milwaukee brace. J Bone Joint Surg Am. 1980;62:599–612. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
