

Amyloidosis of the gastrointestinal tract: a 13-year, single-center, referral experience
- PMID: 22733017
- PMCID: PMC3533676
- DOI: 10.3324/haematol.2012.068155
Amyloidosis of the gastrointestinal tract: a 13-year, single-center, referral experience
Abstract
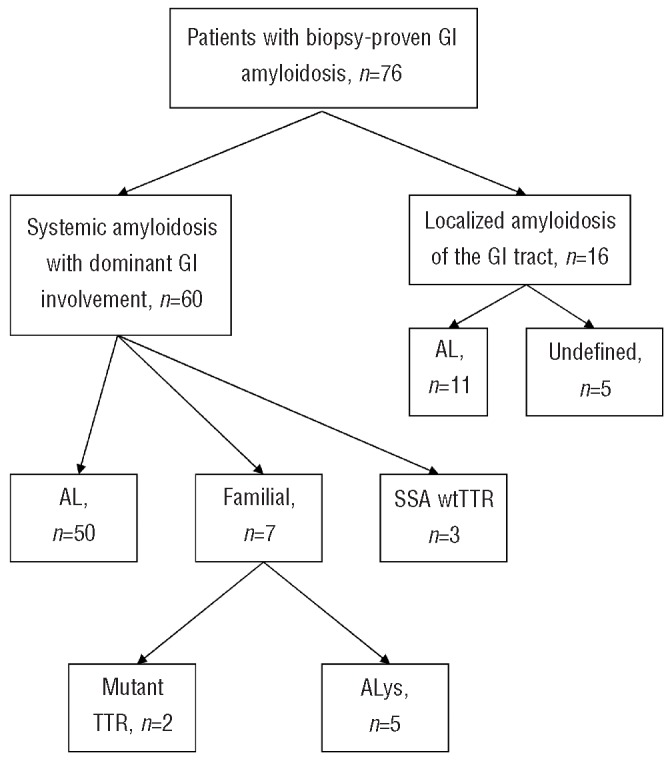
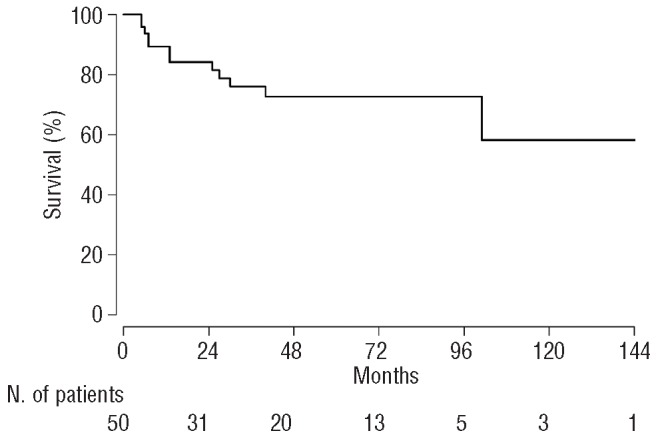
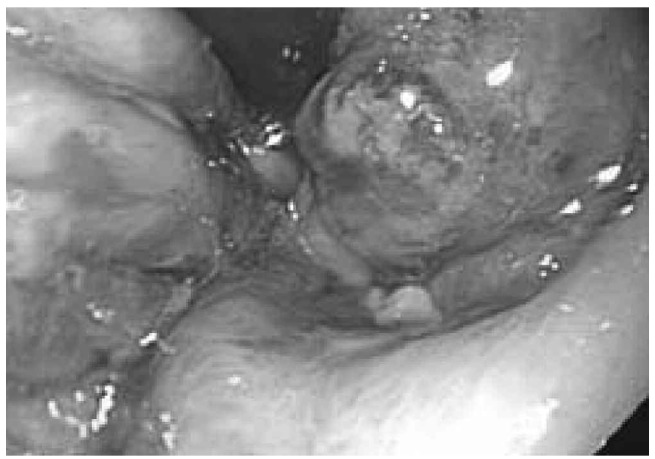
Amyloidosis of the gastrointestinal tract, with biopsy-proven disease, is rare. We reviewed a series of patients who presented with biopsy-proven gastrointestinal amyloidosis and report their clinical characteristics, treatments, and survival. This is a retrospective review of data prospectively collected from January 1998 to December 2011 in a tertiary referral center; 2,334 patients with all types of amyloidosis were evaluated during this period. Seventy-six patients (3.2%) had biopsy-proven amyloid involvement of the gastrointestinal tract. Their median age was 61 years (range, 34-79). Systemic amyloidosis with dominant gastrointestinal involvement was present in 60 (79%) patients, whereas the other 16 (21%) patients had amyloidosis localized to the gastrointestinal tract without evidence of an associated plasma cell dyscrasia or other organ involvement. Of the 60 systemic cases, 50 (83%) had immunoglobulin light-chain, five (8%) had familial lysozyme, three (5%) had wild-type transthyretin, and two (3%) had mutant transthyretin amyloidosis. The most frequent symptoms for all patients were weight loss in 33 (45%) and gastrointestinal bleeding in 27 (36%). Incidental identification of amyloidosis on routine endoscopic surveillance played a role in the diagnosis of seven patients with systemic immunoglobulin light-chain, and four patients with immunoglobulin light-chain localized to the gastrointestinal tract. Amyloid protein subtyping was performed in 12 of the cases of localized disease, and all had lambda light chain disease. Of the 50 patients with systemic immunoglobulin light-chain amyloidosis, 45 were treated with anti-plasma cell therapy. The median survival has not been reached for this group. For the 16 patients with localized gastrointestinal amyloidosis, supportive care was the mainstay of treatment; none received anti-plasma cell therapy. All 16 are alive at a median follow-up of 36 months (range, 1-143). Patients with biopsy-proven gastrointestinal amyloidosis often present with weight loss and bleeding. In localized cases, all that underwent typing were due to lambda light chain amyloidosis and none progressed to systemic disease during the period of follow-up. Most patients with systemic disease had immunoglobulin light-chain, and their tolerance of therapy and median survival were excellent. Although a rare manifestation of amyloidosis, staining for amyloid should be considered in patients undergoing gastrointestinal biopsy who have unexplained chronic gastrointestinal symptoms.
Trial registration: ClinicalTrials.gov NCT00898235.
Figures

References
-
- Merlini G, Bellotti V. Molecular mechanisms of amyloidosis. N Engl J Med. 2003; 349(6):583-96 - PubMed
-
- Sattianayagam PT, Hawkins PN, Gillmore JD. Systemic amyloidosis and the gastrointestinal tract. Nat Rev Gastroenterol Hepatol. 2009;6(10):608-17 - PubMed
-
- Sipe JD, Benson MD, Buxbaum JN, Ikeda S, Merlini G, Saraiva MJ, et al. Amyloid fibril protein nomenclature: 2010 recommendations from the nomenclature committee of the International Society of Amyloidosis. Amyloid. 2010;17(3-4):101-4 - PubMed
-
- Dember LM. Emerging treatment approaches for the systemic amyloidoses. Kidney Int. 2005;68(3):1377-90 - PubMed
-
- Westermark P, Benson MD, Buxbaum JN, Cohen AS, Frangione B, Ikeda S, et al. A primer of amyloid nomenclature. Amyloid. 2007;14(3):179-83 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
