

Hospital-based medication reconciliation practices: a systematic review
- PMID: 22733210
- PMCID: PMC3575731
- DOI: 10.1001/archinternmed.2012.2246
Hospital-based medication reconciliation practices: a systematic review
Abstract
Background: Medication discrepancies at care transitions are common and lead to patient harm. Medication reconciliation is a strategy to reduce this risk.
Objectives: To summarize available evidence on medication reconciliation interventions in the hospital setting and to identify the most effective practices.
Data sources: MEDLINE (1966 through February 2012) and a manual search of article bibliographies.
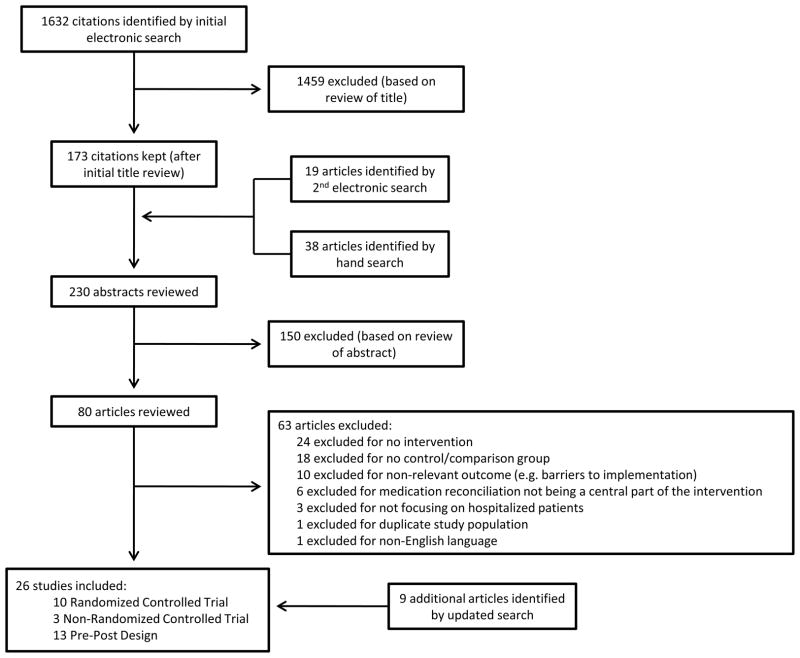
Study selection: Twenty-six controlled studies.
Data extraction: Data were extracted on study design, setting, participants, inclusion/exclusion criteria, intervention components, timing, comparison group, outcome measures, and results.
Data synthesis: Studies were grouped by type of medication reconciliation intervention-pharmacist related, information technology (IT), or other-and were assigned quality ratings using US Preventive Services Task Force criteria.
Results: Fifteen of 26 studies reported pharmacist-related interventions, 6 evaluated IT interventions, and 5 studied other interventions. Six studies were classified as good quality. The comparison group for all the studies was usual care; no studies compared different types of interventions. Studies consistently demonstrated a reduction in medication discrepancies (17 of 17 studies), potential adverse drug events (5 of 6 studies), and adverse drug events (2 of 2 studies) but showed an inconsistent reduction in postdischarge health care utilization (improvement in 2 of 8 studies). Key aspects of successful interventions included intensive pharmacy staff involvement and targeting the intervention to a high-risk patient population.
Conclusions: Rigorously designed studies comparing different inpatient medication reconciliation practices and their effects on clinical outcomes are scarce. Available evidence supports medication reconciliation interventions that heavily use pharmacy staff and focus on patients at high risk for adverse events. Higher-quality studies are needed to determine the most effective approaches to inpatient medication reconciliation.
Comment in
-
Medication reconciliation: moving forward.Arch Intern Med. 2012 Jul 23;172(14):1069-70. doi: 10.1001/archinternmed.2012.2667. Arch Intern Med. 2012. PMID: 22733283 No abstract available.
-
Medication reconciliation practices and potential clinical impact of unintentional discrepancies.JAMA Intern Med. 2013 Feb 11;173(3):246-7. doi: 10.1001/jamainternmed.2013.1235. JAMA Intern Med. 2013. PMID: 23400661 No abstract available.
References
-
- Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE Prevention Study Group. Jama. 1995;274(1):29–34. - PubMed
-
- Krahenbuhl-Melcher A, Schlienger R, Lampert M, Haschke M, Drewe J, Krahenbuhl S. Drug-related problems in hospitals: a review of the recent literature. Drug Saf. 2007;30(5):379–407. - PubMed
-
- Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998 Apr 15;279(15):1200–1205. - PubMed
-
- Coleman EA, Smith JD, Raha D, Min SJ. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med. 2005 Sep 12;165(16):1842–1847. - PubMed
-
- Smith JD, Coleman EA, Min SJ. A new tool for identifying discrepancies in postacute medications for community-dwelling older adults. Am J Geriatr Pharmacother. 2004 Jun;2(2):141–147. - PubMed
