

Rectal imaging: part 1, High-resolution MRI of carcinoma of the rectum at 3 T
- PMID: 22733930
- PMCID: PMC3663716
- DOI: 10.2214/AJR.11.8134
Rectal imaging: part 1, High-resolution MRI of carcinoma of the rectum at 3 T
Abstract
Objective: MRI is currently the imaging modality of choice for the detection, characterization, and staging of rectal cancer. A variety of examinations have been used for preoperative staging of rectal cancer, including digital rectal examination, endorectal (endoscopic) ultrasound, CT, and MRI. Endoscopic ultrasound is the imaging modality of choice for small and small superficial tumors. MRI is superior to CT for assessing invasion to adjacent organs and structures, especially low tumors that carry a high risk of recurrence.
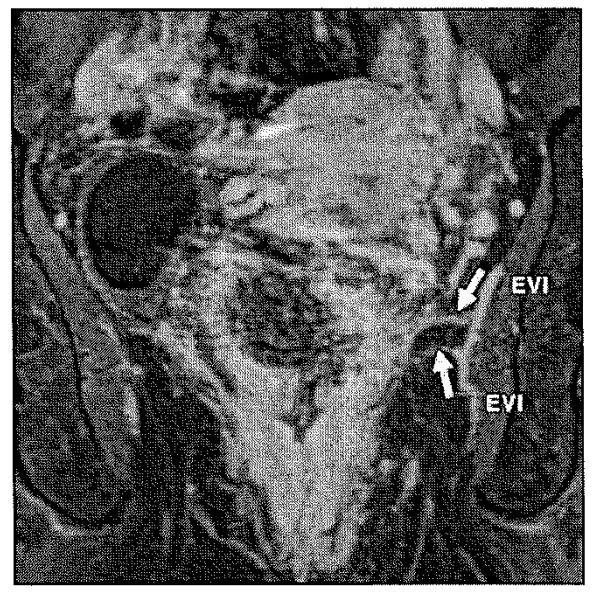
Conclusion: High-resolution MRI is an accurate and sensitive imaging method delineating tumoral margins, mesorectal involvement, nodes, and distant metastasis. In this article, we will review the utility of rectal MRI in local staging, preoperative evaluation, and surgical planning. MRI at 3 T can accurately delineate the mesorectal fascia involvement, which is one of the main decision points in planning treatment.
Figures
References
-
- American Cancer Society . Cancer facts & figures 2011. American Cancer Society; Atlanta, GA: 2011.
-
- Shihab OC, Moran BJ, Heald RJ, Quirke P, Brown G. MRI staging of low rectal cancer. Eur Radial. 2009;19:643–650. - PubMed
-
- Vliegen RF, Beets GL, Lammering G, et al. Mesorectal fascia invasion after neoadjuvant chemotherapy and radiation therapy for locally advanced rectal cancer: accuracy of MR imaging for prediction. Radiology. 2008;246:454–462. - PubMed
-
- Williamson PR, Hellinger MD, Larach SW, Ferrara A. Endorectal ultrasound of T3 and T4 rectal cancers after preoperative chemoradiation. Dis Colon Rectum. 1996;39:45–49. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
