

Patterns of failure after multimodal treatments for high-grade glioma: effectiveness of MIB-1 labeling index
- PMID: 22734595
- PMCID: PMC3583446
- DOI: 10.1186/1748-717X-7-104
Patterns of failure after multimodal treatments for high-grade glioma: effectiveness of MIB-1 labeling index
Abstract
Background: The purpose of the present study was to analyze the recurrence pattern of high-grade glioma treated with a multimodal treatment approach and to evaluate whether the MIB-1 labeling index (LI) could be a useful marker for predicting the pattern of failure in glioblastoma (GB).
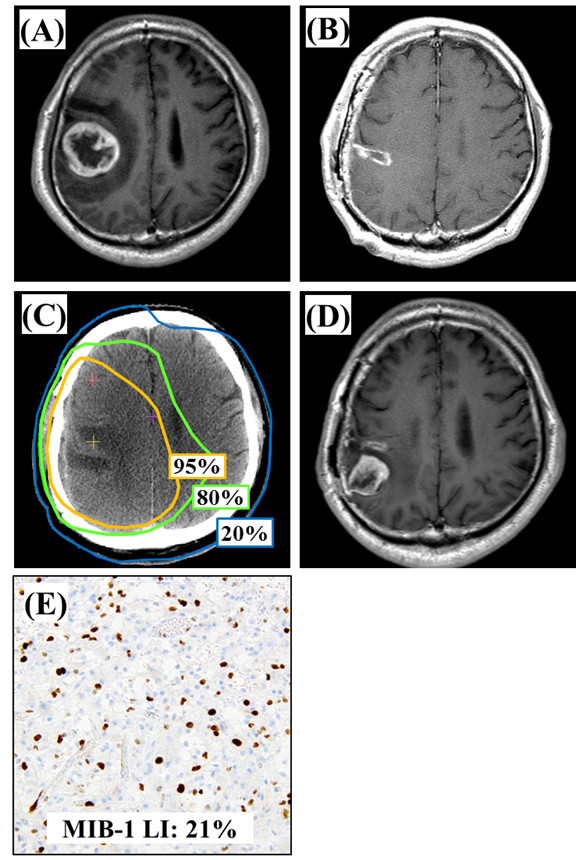
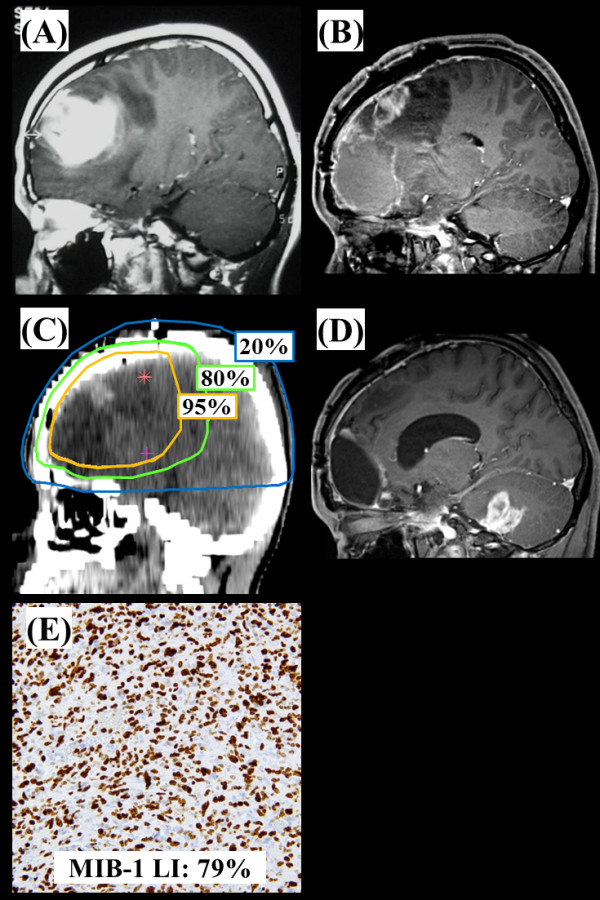
Methods and materials: We evaluated histologically confirmed 131 patients with either anaplastic astrocytoma (AA) or GB. A median dose was 60 Gy. Concomitant and adjuvant chemotherapy were administered to 111 patients. MIB-1 LI was assessed by immunohistochemistry. Recurrence patterns were categorized according to the areas of recurrence as follows: central failure (recurrence in the 95% of 60 Gy); in-field (recurrence in the high-dose volume of 50 Gy; marginal (recurrence outside the high-dose volume) and distant (recurrence outside the RT field).
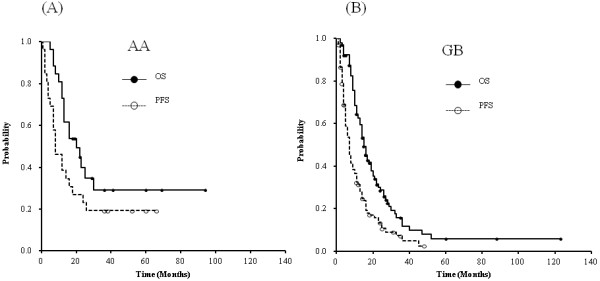
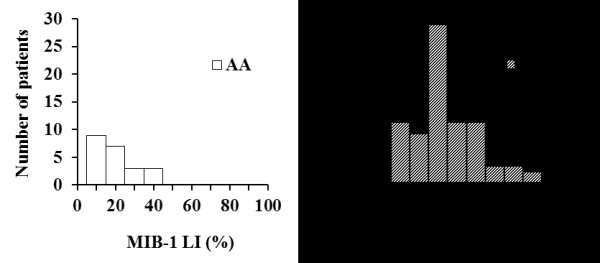
Results: The median follow-up durations were 13 months for all patients and 19 months for those remaining alive. Among AA patients, the 2-year progression-free and overall survival rates were 23.1% and 39.2%, respectively, while in GB patients, the rates were 13.3% and 27.6%, respectively. The median survival time was 20 months for AA patients and 15 months for GB patients. Among AA patients, recurrences were central in 68.7% of patients; in-field, 18.8%; and distant, 12.5%, while among GB patients, 69.0% of recurrences were central, 15.5% were in-field, 12.1% were marginal, and 3.4% were distant. The MIB-1 LI medians were 18.2% in AA and 29.8% in GB. Interestingly, in patients with GB, the MIB-1 LI had a strong effect on the pattern of failure (P = 0.014), while the extent of surgical removal (P = 0.47) and regimens of chemotherapy (P = 0.57) did not.
Conclusions: MIB-1 LI predominantly affected the pattern of failure in GB patients treated with a multimodal approach, and it might be a useful tool for the management of the disease.
Figures
Similar articles
-
Clinicopathological features, MIB-1 labeling index and apoptotic index in recurrent astrocytic tumors.Pathol Oncol Res. 2001;7(4):267-78. doi: 10.1007/BF03032383. Pathol Oncol Res. 2001. PMID: 11882906
-
Solitary fibrous tumor of the central nervous system: a clinicopathologic study of 24 cases.Acta Neurochir (Wien). 2012 Feb;154(2):237-48; discussion 248. doi: 10.1007/s00701-011-1160-9. Epub 2011 Sep 22. Acta Neurochir (Wien). 2012. PMID: 21938461
-
Proposed therapeutic strategy for adult low-grade glioma based on aggressive tumor resection.Neurosurg Focus. 2015 Jan;38(1):E7. doi: 10.3171/2014.10.FOCUS14651. Neurosurg Focus. 2015. PMID: 25599276
-
The clinical value of Ki-67/MIB-1 labeling index in human astrocytomas.Pathol Oncol Res. 2006;12(3):143-7. doi: 10.1007/BF02893360. Epub 2006 Sep 23. Pathol Oncol Res. 2006. PMID: 16998593 Review.
-
Radiation-induced meningiomas in multiple regions, showing rapid recurrence and a high MIB 1 labeling index: a case report and review of the literature.World J Surg Oncol. 2014 Apr 26;12:123. doi: 10.1186/1477-7819-12-123. World J Surg Oncol. 2014. PMID: 24767145 Free PMC article. Review.
Cited by
-
A Prospective Study of Intensity-modulated Radiation Therapy Using a Standard Radiation Dose for High-grade Glioma.Cancer Diagn Progn. 2023 Jul 3;3(4):491-497. doi: 10.21873/cdp.10245. eCollection 2023 Jul-Aug. Cancer Diagn Progn. 2023. PMID: 37405214 Free PMC article.
-
Malignant Endo-suprasellar Glioma: A Case Report and a Brief Review of the Literature.Int J Endocrinol Metab. 2022 Mar 9;20(1):e121803. doi: 10.5812/ijem.121803. eCollection 2022 Jan. Int J Endocrinol Metab. 2022. PMID: 35432550 Free PMC article.
-
Extraneural recurrence of an intracranial nongerminomatous germ cell tumor to cervical lymph nodes in a pediatric patient: Case report.Cancer Rep (Hoboken). 2022 Aug;5(8):e1586. doi: 10.1002/cnr2.1586. Epub 2021 Nov 18. Cancer Rep (Hoboken). 2022. PMID: 34796700 Free PMC article.
-
Analysis of equivalent uniform dose (EUD) and conventional radiation treatment parameters after primary and re-irradiation of malignant glioma.Radiat Oncol. 2013 Dec 13;8:287. doi: 10.1186/1748-717X-8-287. Radiat Oncol. 2013. PMID: 24330746 Free PMC article.
-
Functional Change of Effector Tumor-Infiltrating CCR5+CD38+HLA-DR+CD8+ T Cells in Glioma Microenvironment.Front Immunol. 2019 Oct 9;10:2395. doi: 10.3389/fimmu.2019.02395. eCollection 2019. Front Immunol. 2019. PMID: 31649684 Free PMC article.
References
-
- Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn U, Curschmann J, Janzer RC, Ludwin SK, Mirimanoff RO. et al.Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–996. doi: 10.1056/NEJMoa043330. - DOI - PubMed
-
- Chang EL, Akyurek S, Avalos T, Rebueno N, Spicer C, Garcia J, Famiglietti R, Allen PK, Chao KS, Mahajan A, Woo SY, Maor MH. Evaluation of peritumoral edema in the delineation of radiotherapy clinical target volumes for glioblastoma. Int J Radiat Oncol Biol Phys. 2007;68:144–150. doi: 10.1016/j.ijrobp.2006.12.009. - DOI - PubMed
-
- Lee SW, Fraass BA, Marsh LH, Herbort K, Gebarski SS, Martel MK, Radany EH, Lichter AS, Sandler HM. Patterns of failure following high-dose 3-D conformal radiotherapy for high-grade astrocytomas: A quantitative dosimetric study. Int J Radiat Oncol Biol Phys. 1999;43:79–88. doi: 10.1016/S0360-3016(98)00266-1. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
