

Cell-intrinsic functional effects of the α-cardiac myosin Arg-403-Gln mutation in familial hypertrophic cardiomyopathy
- PMID: 22735528
- PMCID: PMC3379014
- DOI: 10.1016/j.bpj.2012.04.049
Cell-intrinsic functional effects of the α-cardiac myosin Arg-403-Gln mutation in familial hypertrophic cardiomyopathy
Abstract
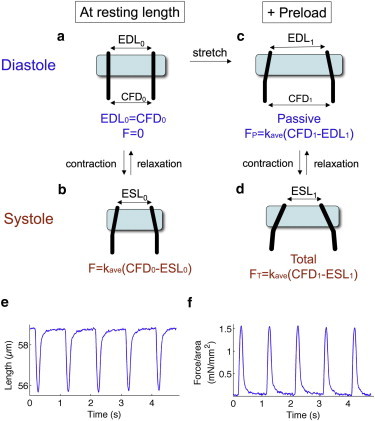
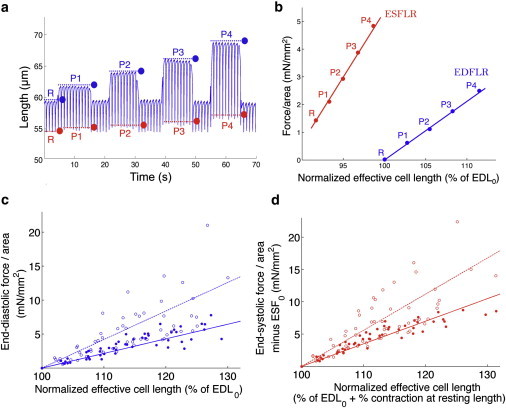
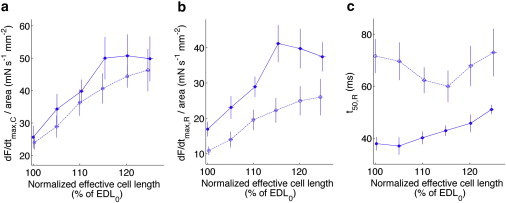
Human familial hypertrophic cardiomyopathy is the most common Mendelian cardiovascular disease worldwide. Among the most severe presentations of the disease are those in families heterozygous for the mutation R403Q in β-cardiac myosin. Mice heterozygous for this mutation in the α-cardiac myosin isoform display typical familial hypertrophic cardiomyopathy pathology. Here, we study cardiomyocytes from heterozygous 403/+ mice. The effects of the R403Q mutation on force-generating capabilities and dynamics of cardiomyocytes were investigated using a dual carbon nanofiber technique to measure single-cell parameters. We demonstrate the Frank-Starling effect at the single cardiomyocyte level by showing that cell stretch causes an increase in amplitude of contraction. Mutant 403/+ cardiomyocytes exhibit higher end-diastolic and end-systolic stiffness than +/+ cardiomyocytes, whereas active force generation capabilities remain unchanged. Additionally, 403/+ cardiomyocytes show slowed relaxation dynamics. These phenotypes are consistent with increased end-diastolic and end-systolic chamber elastance, as well as diastolic dysfunction seen at the level of the whole heart. Our results show that these functional effects of the R403Q mutation are cell-intrinsic, a property that may be a general phenomenon in familial hypertrophic cardiomyopathy.
Copyright © 2012 Biophysical Society. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Maron B.J., Gardin J.M., Bild D.E. Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the CARDIA Study. Coronary Artery Risk Development in (Young) Adults. Circulation. 1995;92:785–789. - PubMed
-
- Maron B.J. Hypertrophic cardiomyopathy: a systematic review. JAMA. 2002;287:1308–1320. - PubMed
-
- Maron B.J., Spirito P., Arce J. Noninvasive assessment of left ventricular diastolic function by pulsed Doppler echocardiography in patients with hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 1987;10:733–742. - PubMed
-
- Epstein N.D., Cohn G.M., Fananapazir L. Differences in clinical expression of hypertrophic cardiomyopathy associated with two distinct mutations in the beta-myosin heavy chain gene. A 908-Leu----Val mutation and a 403-Arg----Gln mutation. Circulation. 1992;86:345–352. - PubMed
-
- Geisterfer-Lowrance A.A., Kass S., Seidman J.G. A molecular basis for familial hypertrophic cardiomyopathy: a beta cardiac myosin heavy chain gene missense mutation. Cell. 1990;62:999–1006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
