

Metronomic chemotherapy in combination with antiangiogenic treatment induces mosaic vascular reduction and tumor growth inhibition in hepatocellular carcinoma xenografts
- PMID: 22736027
- PMCID: PMC11824204
- DOI: 10.1007/s00432-012-1270-7
Metronomic chemotherapy in combination with antiangiogenic treatment induces mosaic vascular reduction and tumor growth inhibition in hepatocellular carcinoma xenografts
Abstract
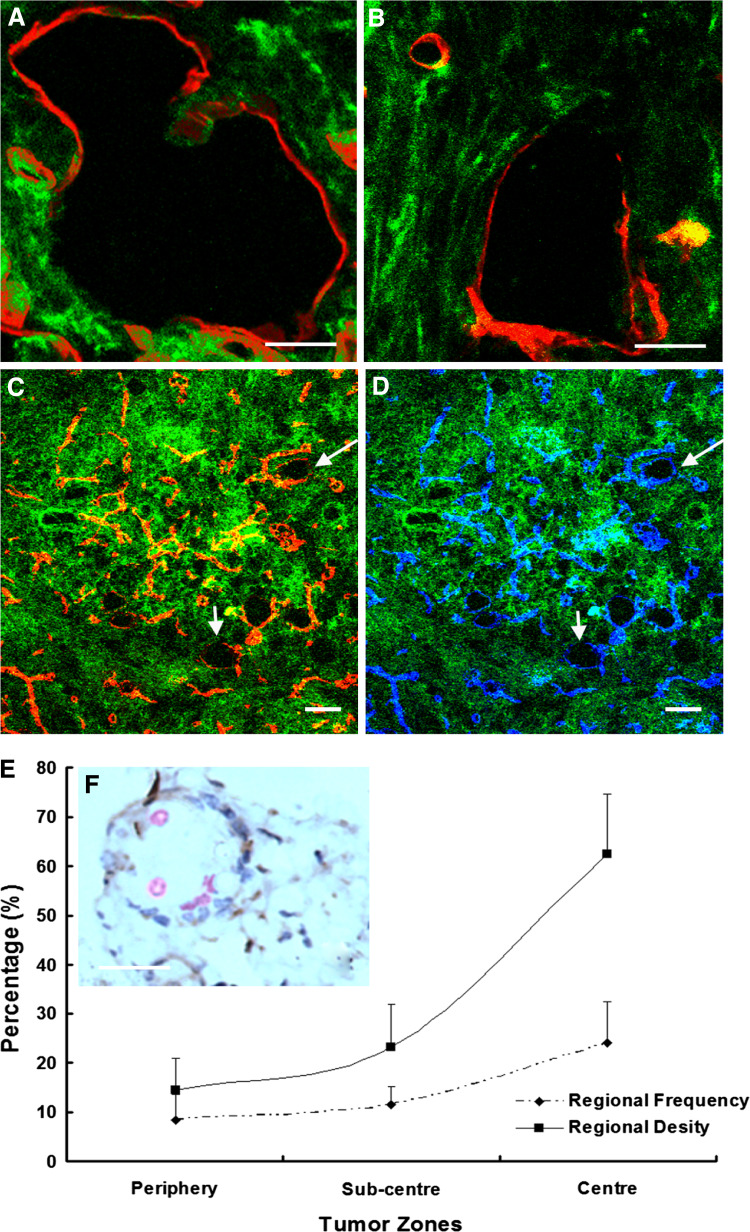
Background: In addition to sprouting angiogenesis, other mechanisms, such as mosaic tumor vessel formation, have been recognized to contribute to tumor vascularization. We sought to examine vascular alteration as well as tumor growth inhibition after treatment with antiangiogenic therapy, chemotherapy alone or in combination.
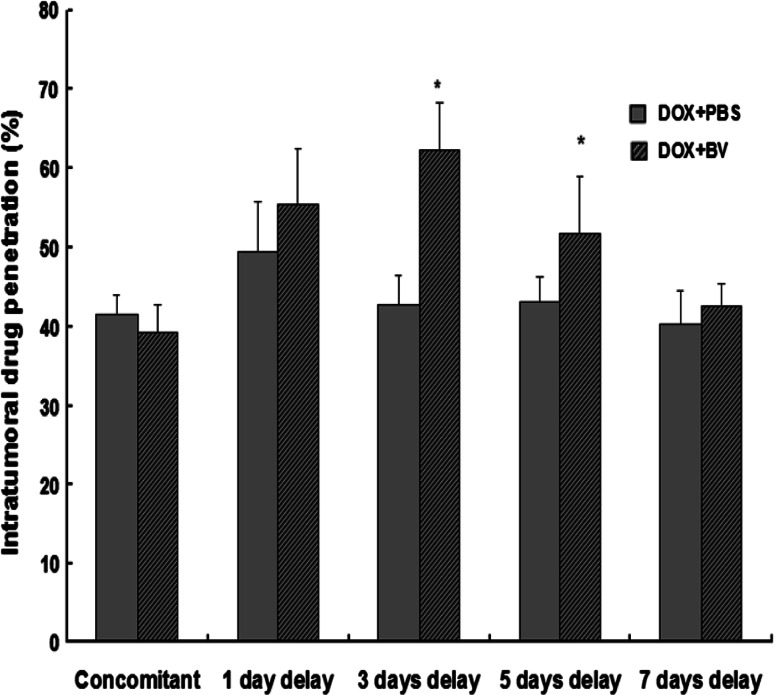
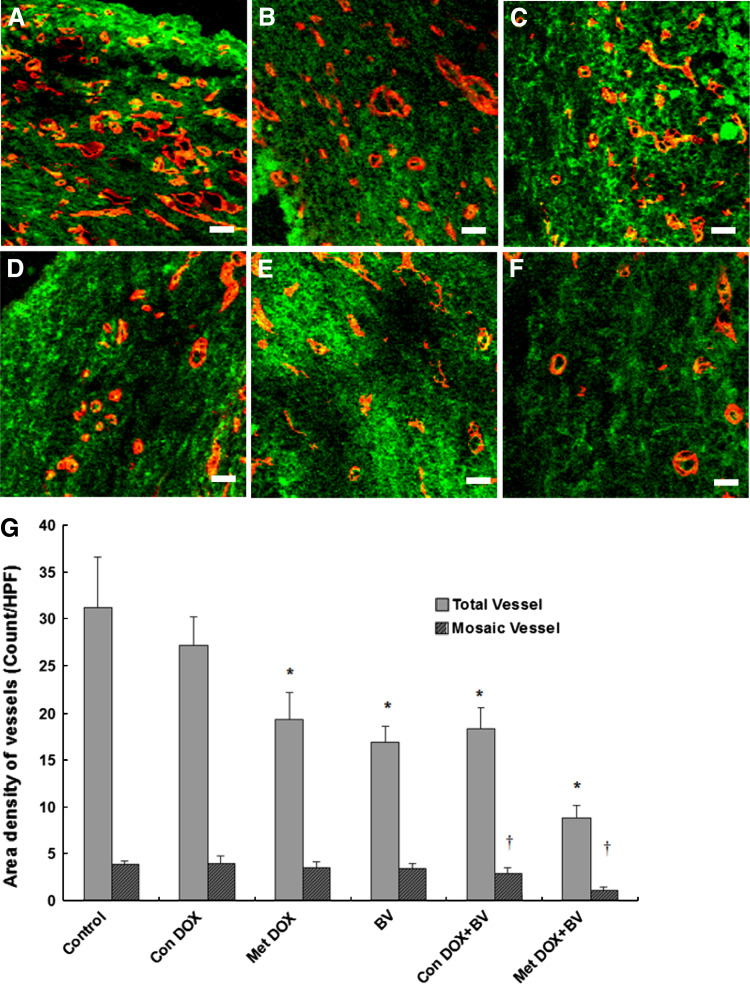
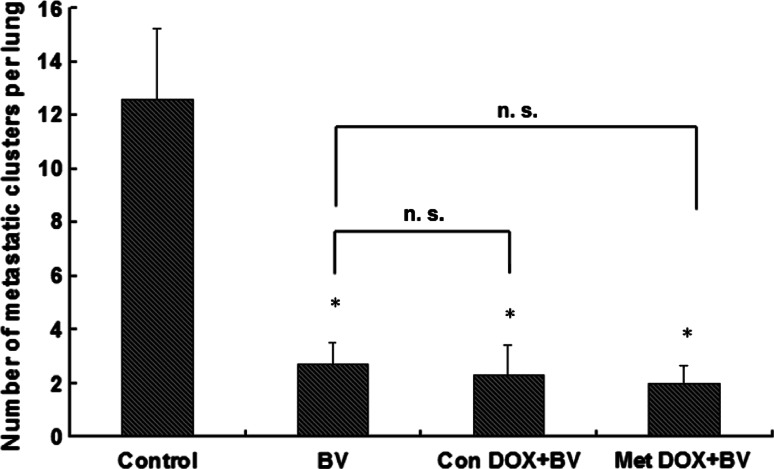
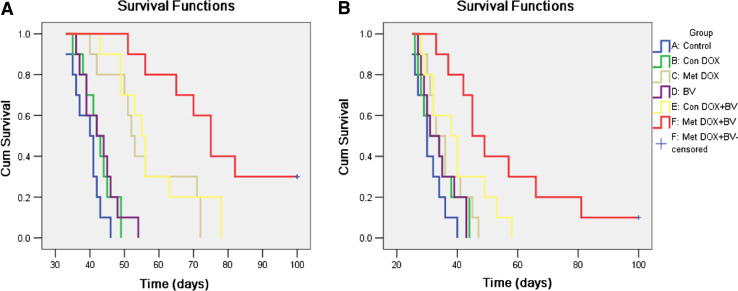
Methods: Hepatocellular carcinoma cells (Hep3B) expressed green fluorescent protein were utilized to establish orthotopic xenograft model in nude mice. The formation and distribution of mosaic vessels was analyzed quantitatively by immunolabeling. Next, changes in tumor microcirculation and therapeutic effects on tumor growth were evaluated in several different treatment groups: control, conventional doxorubicin, metronomic doxorubicin, bevacizumab, bevacizumab plus conventional doxorubicin, and bevacizumab plus metronomic doxorubicin. In addition, we examined the effects of combined regimens on lung metastasis using a highly metastatic human hepatocellular carcinoma (HCCLM3) mouse model.
Results: Approximately 62 % of the vessels were present in the central part or near the midsection of the tumor and were mosaic. Only the combined antiangiogenic treatment and chemotherapy (metronomic schedule, P = 0.00; conventional schedule, P = 0.02) had a significant effect on the degree of mosaic vasculature. Metronomic doxorubicin in combination with bevacizumab had an even more profound effect than bevacizumab plus conventional doxorubicin (P < 0.05) on tumor growth inhibition and survival. However, bevacizumab plus metronomic doxorubicin failed to inhibit lung metastasis compared with antiangiogenic monotherapy.
Conclusions: Metronomic chemotherapy in combination with antiangiogenic treatment results in the reduction of mosaic tumor vasculature, inhibition of tumor growth, and enhanced survival of mice. Further investigation of drug scheduling is required to optimize antitumor activity.
Conflict of interest statement
We declare that we have no conflict of interest.
Figures
Similar articles
-
Bevacizumab enhances chemosensitivity of hepatocellular carcinoma to adriamycin related to inhibition of survivin expression.J Cancer Res Clin Oncol. 2011 Mar;137(3):505-12. doi: 10.1007/s00432-010-0914-8. Epub 2010 May 21. J Cancer Res Clin Oncol. 2011. PMID: 20490863 Free PMC article.
-
Toripalimab plus bevacizumab versus sorafenib as first-line treatment for advanced hepatocellular carcinoma (HEPATORCH): a randomised, open-label, phase 3 trial.Lancet Gastroenterol Hepatol. 2025 Jul;10(7):658-670. doi: 10.1016/S2468-1253(25)00059-7. Epub 2025 May 20. Lancet Gastroenterol Hepatol. 2025. PMID: 40409323 Clinical Trial.
-
The clinical effectiveness and cost-effectiveness of cetuximab (mono- or combination chemotherapy), bevacizumab (combination with non-oxaliplatin chemotherapy) and panitumumab (monotherapy) for the treatment of metastatic colorectal cancer after first-line chemotherapy (review of technology appraisal No.150 and part review of technology appraisal No. 118): a systematic review and economic model.Health Technol Assess. 2013 Apr;17(14):1-237. doi: 10.3310/hta17140. Health Technol Assess. 2013. PMID: 23547747 Free PMC article.
-
Octreotide acts as an antitumor angiogenesis compound and suppresses tumor growth in nude mice bearing human hepatocellular carcinoma xenografts.J Cancer Res Clin Oncol. 2003 Jun;129(6):327-34. doi: 10.1007/s00432-003-0447-5. Epub 2003 Jun 14. J Cancer Res Clin Oncol. 2003. PMID: 12811549 Free PMC article.
-
Vascular-endothelial-growth-factor (VEGF) targeting therapies for endocrine refractory or resistant metastatic breast cancer.Cochrane Database Syst Rev. 2012 Jul 11;2012(7):CD008941. doi: 10.1002/14651858.CD008941.pub2. Cochrane Database Syst Rev. 2012. PMID: 22786517 Free PMC article.
Cited by
-
Cancer chemotherapy: insights into cellular and tumor microenvironmental mechanisms of action.Front Oncol. 2022 Jul 29;12:960317. doi: 10.3389/fonc.2022.960317. eCollection 2022. Front Oncol. 2022. PMID: 35965519 Free PMC article. Review.
-
Anti-angiogenic agents for the treatment of solid tumors: Potential pathways, therapy and current strategies - A review.J Adv Res. 2017 Nov;8(6):591-605. doi: 10.1016/j.jare.2017.06.006. Epub 2017 Jun 27. J Adv Res. 2017. PMID: 28808589 Free PMC article. Review.
-
Modulation of the tumor vasculature and oxygenation to improve therapy.Pharmacol Ther. 2015 Sep;153:107-24. doi: 10.1016/j.pharmthera.2015.06.006. Epub 2015 Jun 11. Pharmacol Ther. 2015. PMID: 26073310 Free PMC article. Review.
-
Combination therapy in cancer: effects of angiogenesis inhibitors on drug pharmacokinetics and pharmacodynamics.Chin J Cancer. 2016 Jun 29;35(1):61. doi: 10.1186/s40880-016-0123-1. Chin J Cancer. 2016. PMID: 27357621 Free PMC article. Review.
-
Potential of substituted quinazolines to interact with multiple targets in the treatment of cancer.Bioorg Med Chem. 2021 Apr 1;35:116061. doi: 10.1016/j.bmc.2021.116061. Epub 2021 Feb 12. Bioorg Med Chem. 2021. PMID: 33647840 Free PMC article.
References
-
- Abou-Alfa GK, Schwartz L, Ricci S, Amadori D, Santoro A, Figer A, De Greve J, Douillard JY, Lathia C, Schwartz B, Taylor I, Moscovici M, Saltz LB (2006) Phase II study of sorafenib in patients with advanced hepatocellular carcinoma. J Clin Oncol 24(26):4293–4300 - PubMed
-
- Auguste P, Lemiere S, Larrieu-Lahargue F, Bikfalvi A (2005) Molecular mechanisms of tumor vascularization. Crit Rev Oncol Hematol 54(1):53–61 - PubMed
-
- Bocci G, Nicolaou KC, Kerbel RS (2002) Protracted low-dose effects on human endothelial cell proliferation and survival in vitro reveal a selective antiangiogenic window for various chemotherapeutic drugs. Cancer Res 62(23):6938–6943 - PubMed
-
- Browder T, Butterfield CE, Kraling BM, Shi B, Marshall B, O’Reilly MS, Folkman J (2000) Antiangiogenic scheduling of chemotherapy improves efficacy against experimental drug-resistant cancer. Cancer Res 60(7):1878–1886 - PubMed
-
- Bruix J, Hessheimer AJ, Forner A, Boix L, Vilana R, Llovet JM (2006) New aspects of diagnosis and therapy of hepatocellular carcinoma. Oncogene 25(27):3848–3856 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
