

Endothelial cells obtained from patients affected by chronic venous disease exhibit a pro-inflammatory phenotype
- PMID: 22737245
- PMCID: PMC3380919
- DOI: 10.1371/journal.pone.0039543
Endothelial cells obtained from patients affected by chronic venous disease exhibit a pro-inflammatory phenotype
Abstract
Background: The inflammatory properties of vein endothelium in relation to chronic venous disease (CVD) have been poorly investigated. Therefore, new insights on the characteristics of large vein endothelium would increase our knowledge of large vessel physiopathology.
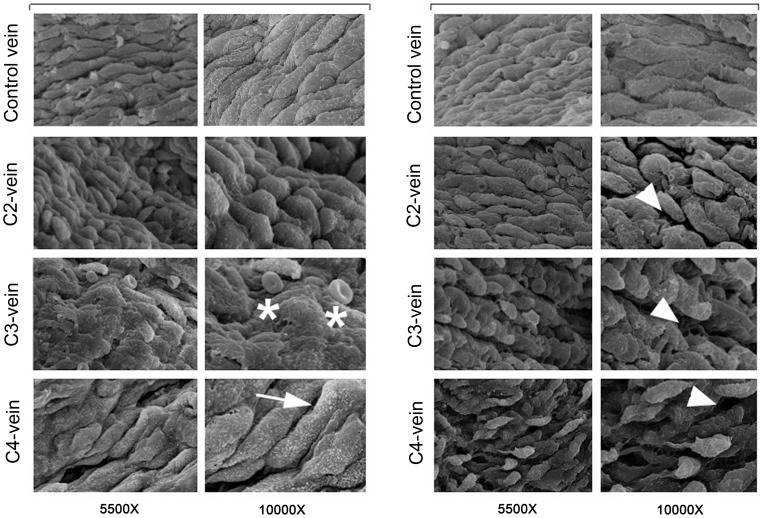
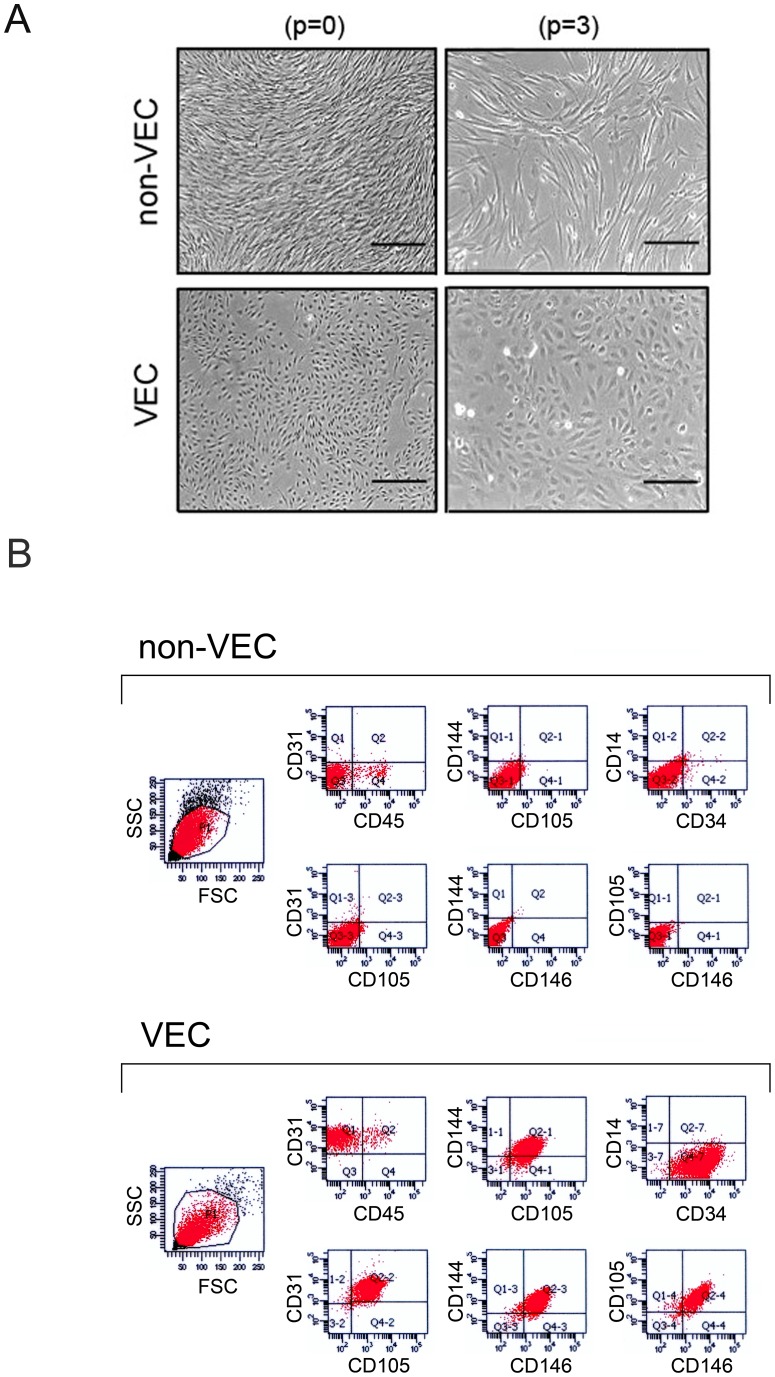
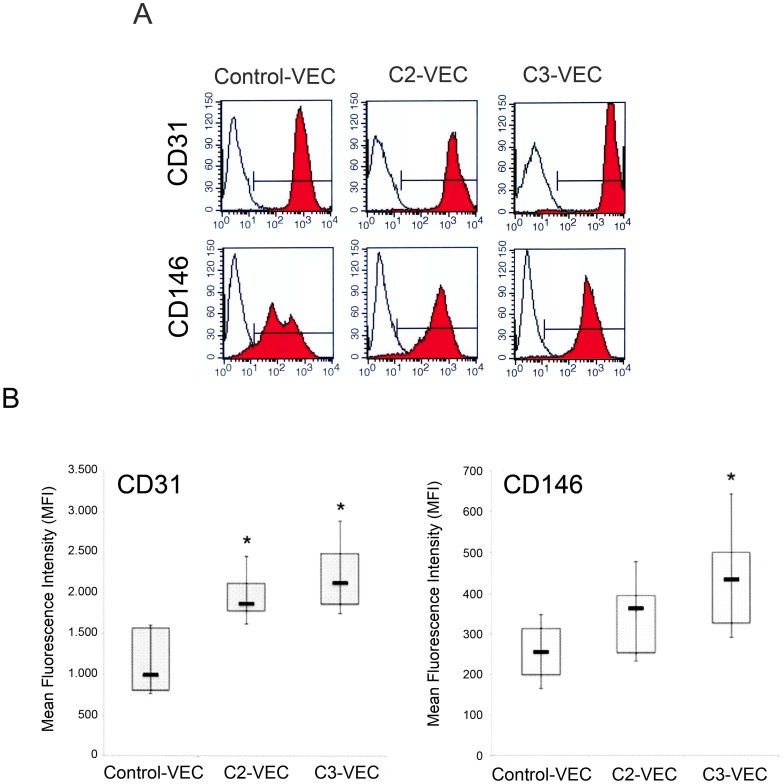
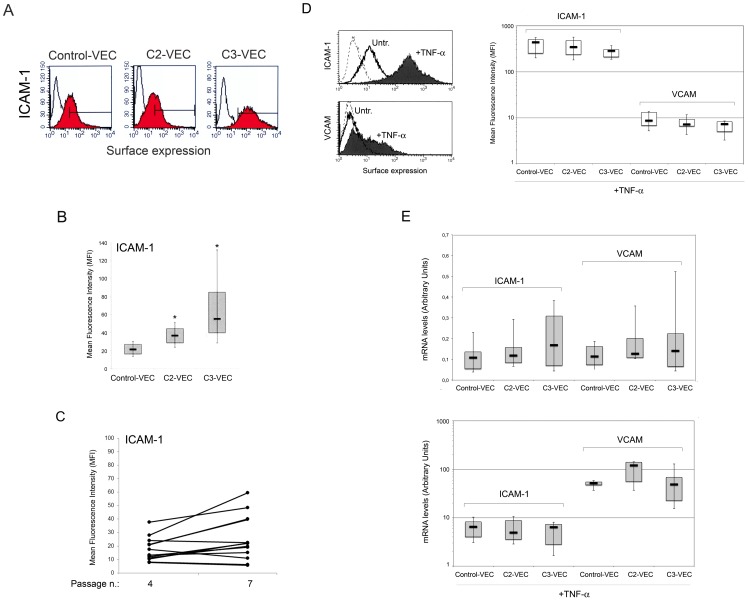
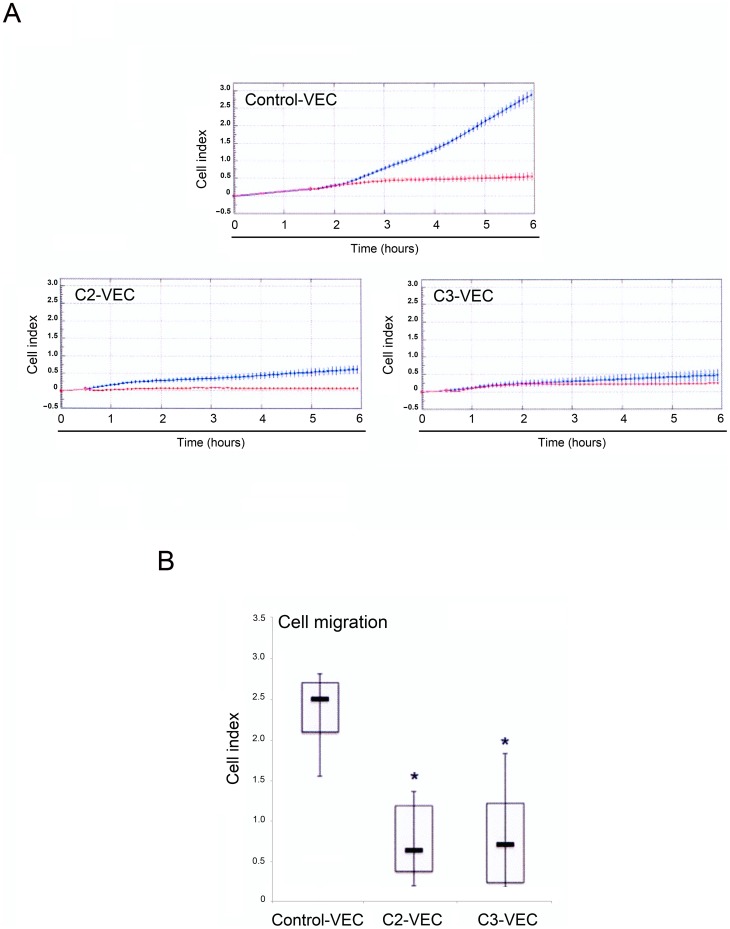
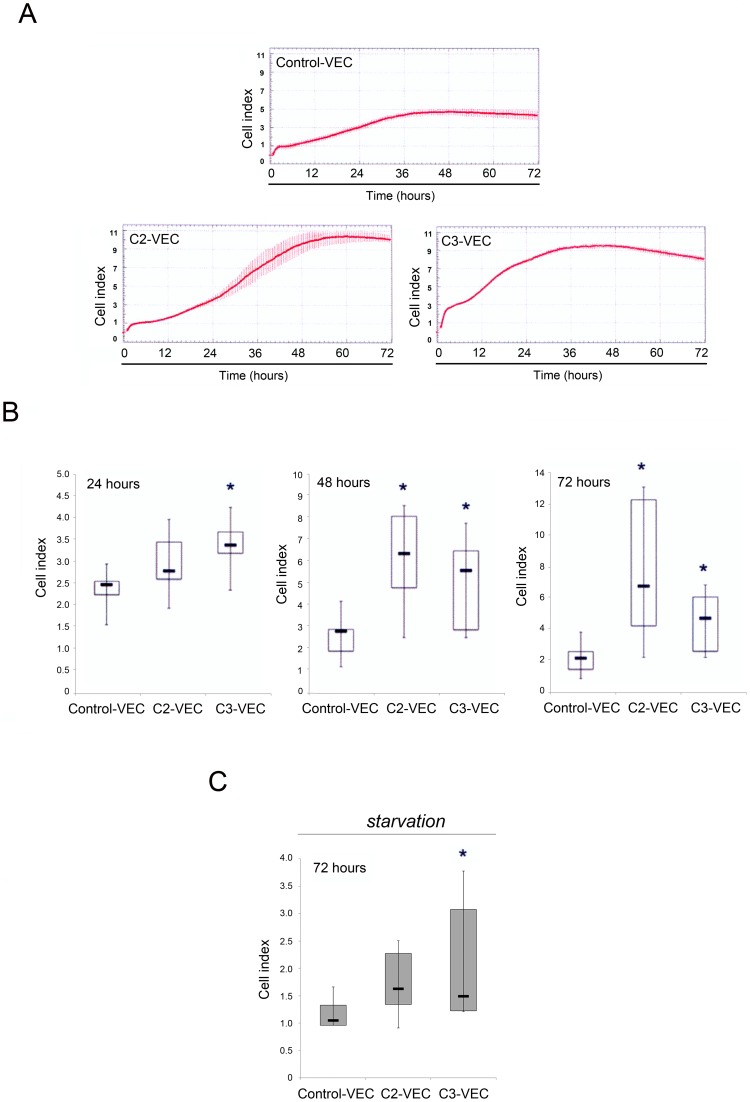
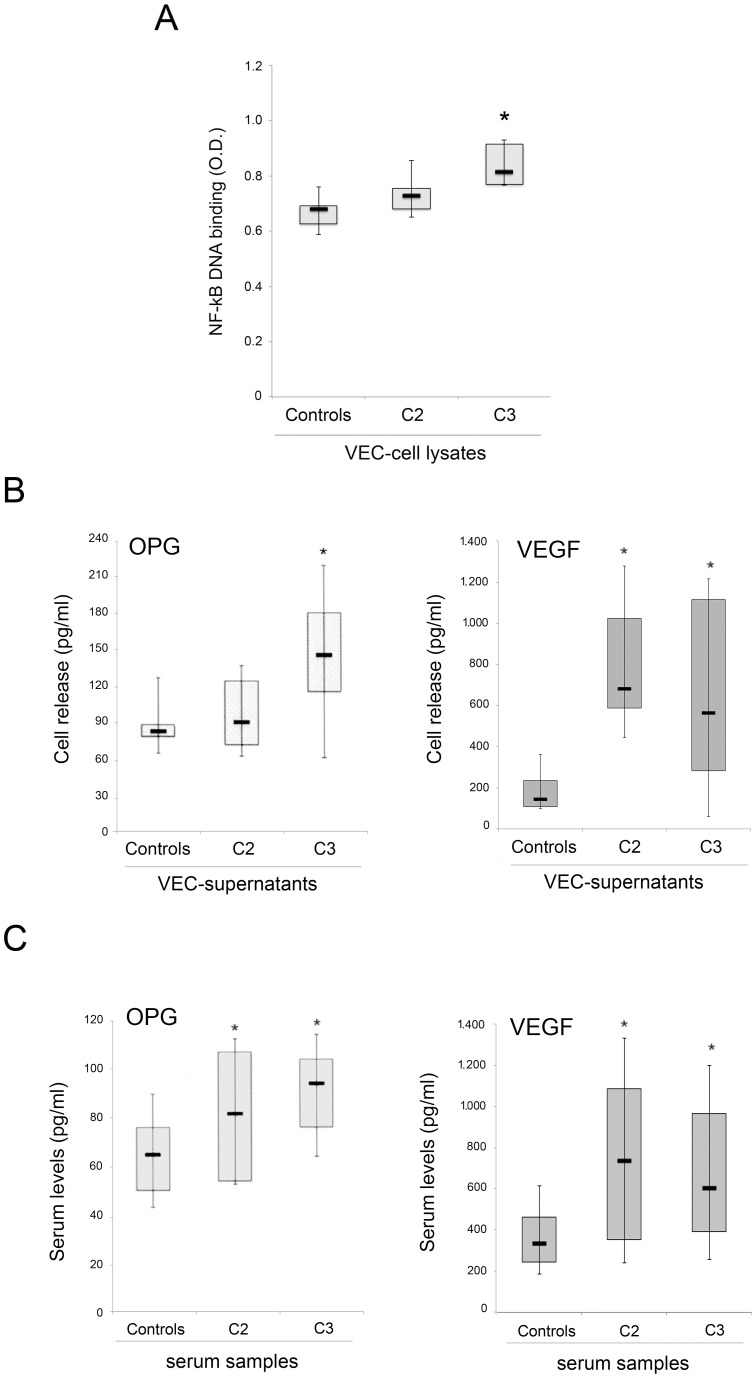
Methodology/principal findings: Surgical specimens of veins were obtained from the tertiary venous network (R3) and/or saphenous vein (SF) of patients affected by CVD and from control individuals. Highly purified venous endothelial cell (VEC) cultures obtained from CVD patients were characterized for morphological, phenotypic and functional properties compared to control VEC. An increase of CD31/PECAM-1, CD146 and ICAM-1 surface levels was documented at flow cytometry in pathological VEC with respect to normal controls. Of note, the strongest expression of these pro-inflammatory markers was observed in VEC obtained from patients with more advanced disease. Similarly, spontaneous cell proliferation and resistance to starvation was higher in pathological than in normal VEC, while the migratory response of VEC showed an opposite trend, being significantly lower in VEC obtained from pathological specimens. In addition, in keeping with a higher baseline transcriptional activity of NF-kB, the release of the pro-inflammatory cytokines osteoprotegerin (OPG) and vascular endothelial growth factor (VEGF) was higher in pathological VEC cultures with respect to control VEC. Interestingly, there was a systemic correlation to these in vitro data, as demonstrated by higher serum OPG and VEGF levels in CVD patients with respect to normal healthy controls.
Conclusion/significance: Taken together, these data indicate that large vein endothelial cells obtained from CVD patients exhibit a pro-inflammatory phenotype, which might significantly contribute to systemic inflammation in CVD patients.
Conflict of interest statement
Figures
References
-
- Eberhardt RT, Raffetto JD. Chronic venous insufficiency. Circulation. 2005;111:2398–2409. - PubMed
-
- Parkington HC, Coleman HA, Tare M. Prostacyclin and endothelium dependent hyperpolarization. Pharmacol Res. 2004;49:509–514. - PubMed
-
- Levi M, Keller TT, van Gorp E, ten Cate H. Infection and inflammation and the coagulation system. Cardiovasc Res. 2003;60:26–39. - PubMed
-
- von Andrian UH, Mackay CR. T-Cell function and migration. Two sides of the same coin. N Engl J Med. 2000;343:1020–1034. - PubMed
-
- Ulbrich H, Eriksson EE, Lindbom L. Leukocyte and endothelial cell adhesion molecules as targets for therapeutic interventions in inflammatory disease. Trends Pharmacol Sci. 2003;24:640–647. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
