

Behavior, nutrition and lifestyle in a comprehensive health and disease paradigm: skills and knowledge for a predictive, preventive and personalized medicine
- PMID: 22738244
- PMCID: PMC3384462
- DOI: 10.1007/s13167-012-0141-2
Behavior, nutrition and lifestyle in a comprehensive health and disease paradigm: skills and knowledge for a predictive, preventive and personalized medicine
Abstract
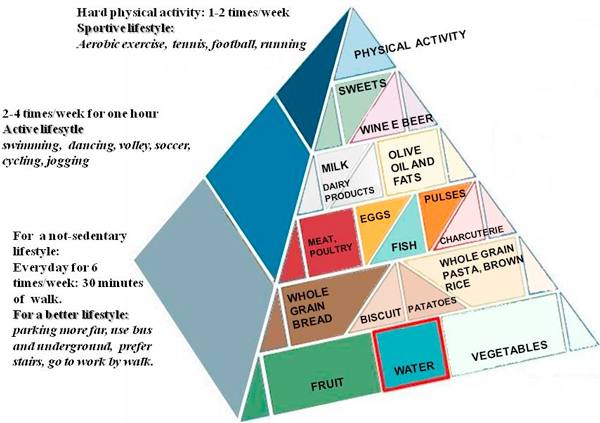
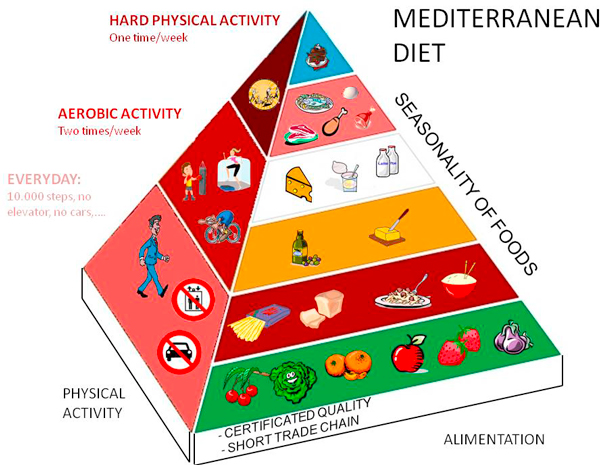
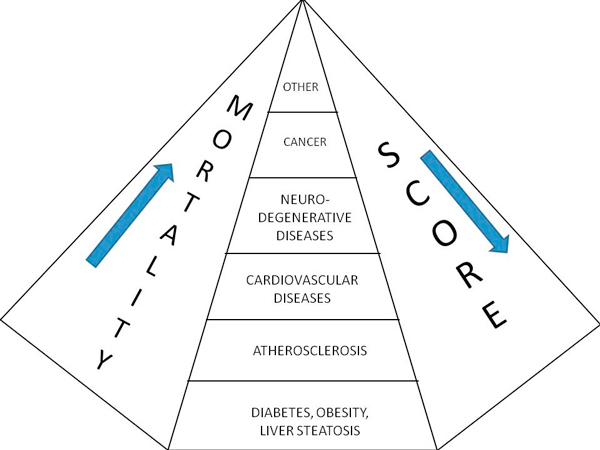
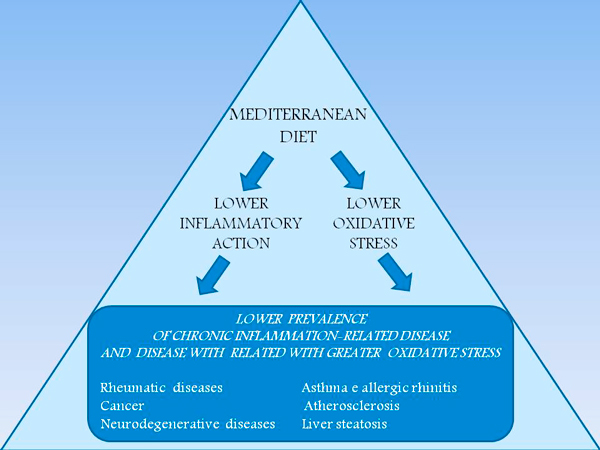
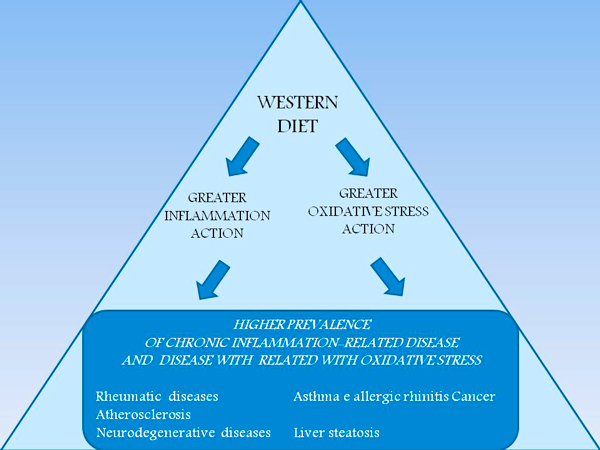
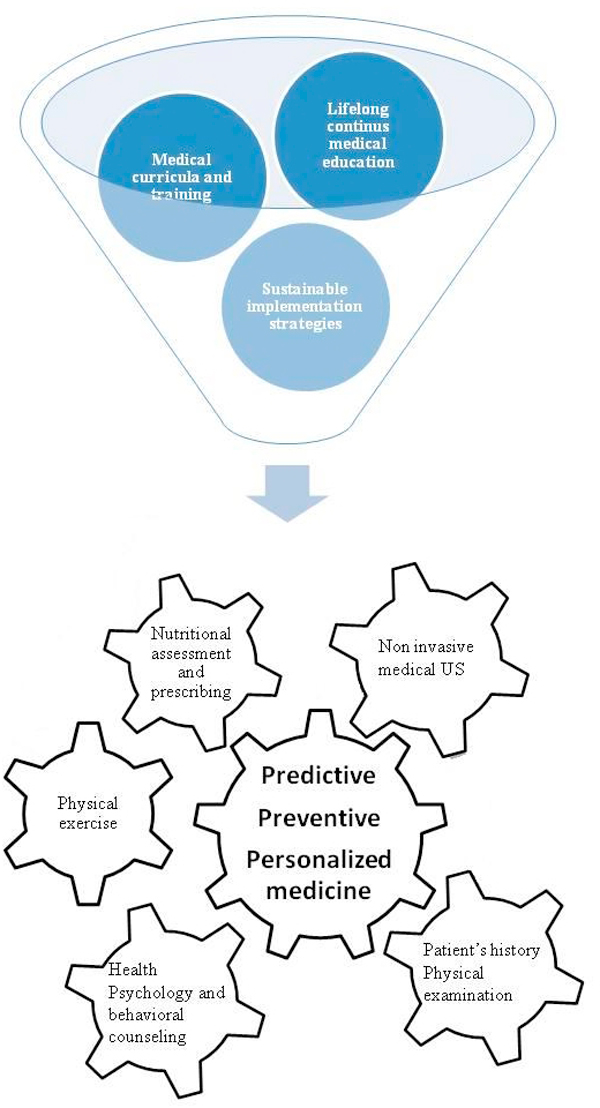
Health and disease of individuals and of populations are the result of three groups of risk factors: genetics, environment and behavior. Assessment, interventions and tailored changes are possible with integrated approaches more effective if respectful of individuals and different cultures. Assessment tools and integrated interventional strategies are available, but widespread knowledge, skills and competence of well trained individual Medical Doctors still lack. Mediterranean diet is an appropriate reference paradigm because encompasses consistent research background, affordable sustainability, widespread comprehensibility and attractiveness inside a cultural framework of competences and skills in which the Medical Doctors can personally manage the need of prediction (early diagnosis), prevention (intervention on healthy persons) and tailored therapy and follow-up for patients. This profile is flexible and adjustable according to specific needs and preferences due to different economic and ethno-cultural milieus. It can enhanced through on-site/e-learning Continuous Medical Education (CME), by training and using friendly and affordable equipments.
Figures

References
-
- Walker ARP. Can expectation of life in western populations be increased by changes in diet and manner of life? S Afr Med J. 1968;42:144–50. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
