

A novel differential diagnostic model based on multiple biological parameters for immunoglobulin A nephropathy
- PMID: 22738421
- PMCID: PMC3488968
- DOI: 10.1186/1472-6947-12-58
A novel differential diagnostic model based on multiple biological parameters for immunoglobulin A nephropathy
Abstract
Background: Immunoglobulin A nephropathy (IgAN) is the most common form of glomerulonephritis in China. An accurate diagnosis of IgAN is dependent on renal biopsies, and there is lack of non-invasive and practical classification methods for discriminating IgAN from other primary kidney diseases. The objective of this study was to develop a classification model for the auxiliary diagnosis of IgAN using multiparameter analysis with various biological parameters.
Methods: To establish an optimal classification model, 121 cases (58 IgAN vs. 63 non-IgAN) were recruited and statistically analyzed. The model was then validated in another 180 cases.
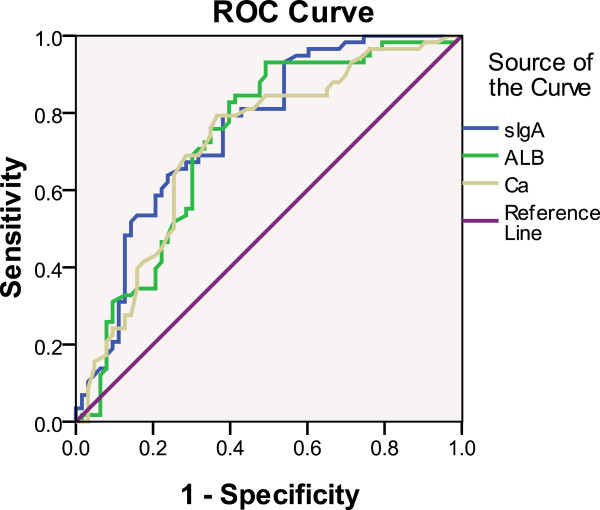
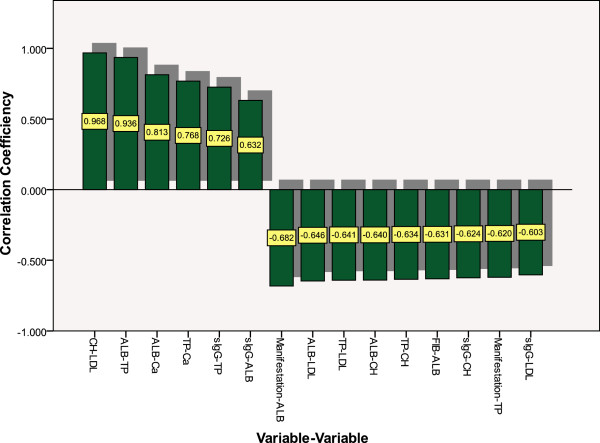
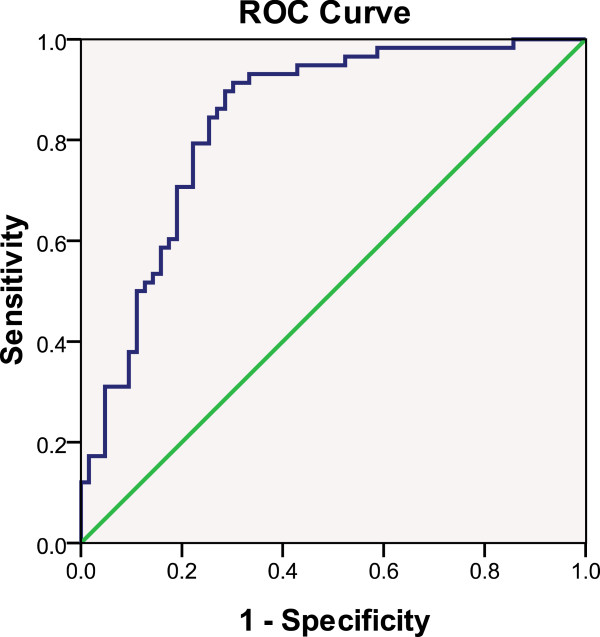
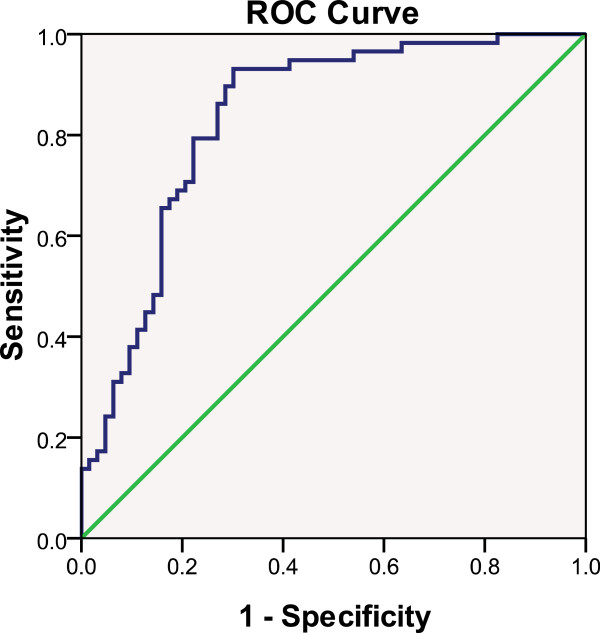
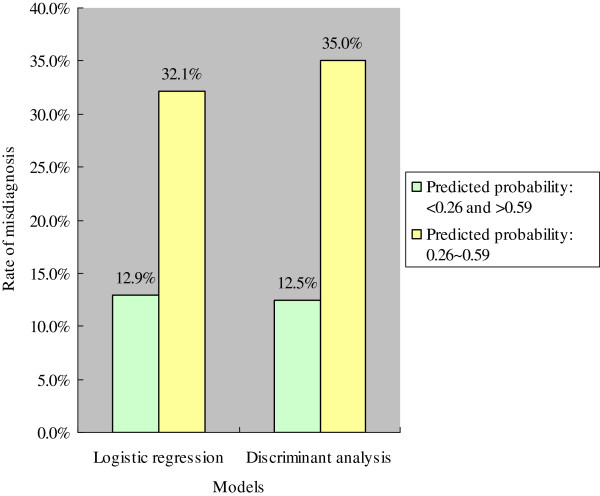
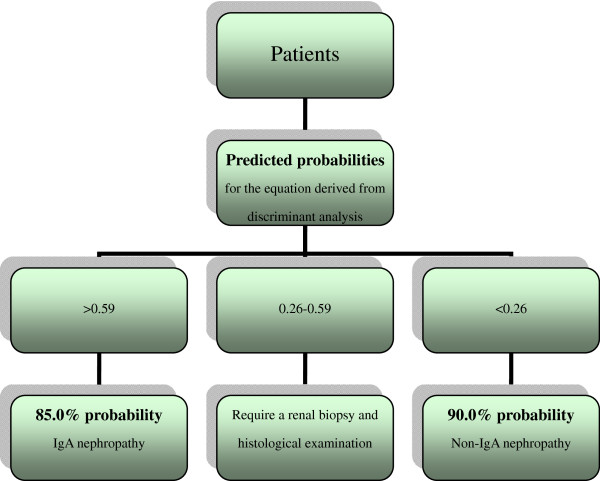
Results: Of the 57 biological parameters, there were 16 parameters that were significantly different (P < 0.05) between IgAN and non-IgAN. The combination of fibrinogen, serum immunoglobulin A level, and manifestation was found to be significant in predicting IgAN. The validation accuracies of the logistic regression and discriminant analysis models were 77.5 and 77.0%, respectively at a predictive probability cut-off of 0.5, and 81.1 and 79.9%, respectively, at a predictive probability cut-off of 0.40. When the predicted probability of the equation containing the combination of fibrinogen, serum IgA level, and manifestation was more than 0.59, a patient had at least an 85.0% probability of having IgAN. When the predicted probability was lower than 0.26, a patient had at least an 88.5% probability of having non-IgAN. The results of the net reclassification improvement certificated serum Immunoglobulin A and fibrinogen had classification power for discriminating IgAN from non-IgAN.
Conclusions: These models possess potential clinical applications in distinguishing IgAN from other primary kidney diseases.
Figures
Similar articles
-
A pilot and comparative study between pathological and serological levels of immunoglobulin and complement among three kinds of primary glomerulonephritis.BMC Immunol. 2018 Jun 20;19(1):18. doi: 10.1186/s12865-018-0254-z. BMC Immunol. 2018. PMID: 29925312 Free PMC article.
-
A non-invasive diagnostic model of immunoglobulin A nephropathy and serological markers for evaluating disease severity.Chin Med J (Engl). 2019 Mar 20;132(6):647-652. doi: 10.1097/CM9.0000000000000121. Chin Med J (Engl). 2019. PMID: 30855344 Free PMC article.
-
High serum IgA/C3 ratio better predicts a diagnosis of IgA nephropathy among primary glomerular nephropathy patients with proteinuria ≤ 1 g/d: an observational cross-sectional study.BMC Nephrol. 2019 Apr 30;20(1):150. doi: 10.1186/s12882-019-1331-0. BMC Nephrol. 2019. PMID: 31039758 Free PMC article.
-
Post-transplant immunoglobulin A deposition and nephropathy in allografts.Nephrology (Carlton). 2018 Jul;23 Suppl 2:4-9. doi: 10.1111/nep.13281. Nephrology (Carlton). 2018. PMID: 29968406 Review.
-
Proliferative glomerulonephritis with monoclonal immunoglobulin G deposits complicated by immunoglobulin A nephropathy in the renal allograft.Nephrology (Carlton). 2016 Jul;21 Suppl 1:48-52. doi: 10.1111/nep.12775. Nephrology (Carlton). 2016. PMID: 26971743 Review.
Cited by
-
Urinary peptide panel for prognostic assessment of bladder cancer relapse.Sci Rep. 2019 May 21;9(1):7635. doi: 10.1038/s41598-019-44129-y. Sci Rep. 2019. PMID: 31114012 Free PMC article.
-
A diagnostic model for minimal change disease based on biological parameters.PeerJ. 2018 Jan 12;6:e4237. doi: 10.7717/peerj.4237. eCollection 2018. PeerJ. 2018. PMID: 29340242 Free PMC article.
-
A noninvasive artificial neural network model to predict IgA nephropathy risk in Chinese population.Sci Rep. 2022 May 18;12(1):8296. doi: 10.1038/s41598-022-11964-5. Sci Rep. 2022. PMID: 35585099 Free PMC article.
-
A pilot and comparative study between pathological and serological levels of immunoglobulin and complement among three kinds of primary glomerulonephritis.BMC Immunol. 2018 Jun 20;19(1):18. doi: 10.1186/s12865-018-0254-z. BMC Immunol. 2018. PMID: 29925312 Free PMC article.
-
Machine learning-based diagnostic prediction of IgA nephropathy: model development and validation study.Sci Rep. 2024 May 30;14(1):12426. doi: 10.1038/s41598-024-63339-7. Sci Rep. 2024. PMID: 38816457 Free PMC article.
References
-
- Appel AS, Appel GB. An update on the use of mycophenolate mofetil in lupus nephritis and other primary glomerular diseases. Nat Clin Pract Nephrol. 2009;5:132–142. - PubMed
-
- Bomback AS, Radhakrishnan J. Treatment of nephrotic syndrome with adrenocorticotropic hormone (ACTH) Discov Med. 2011;12:91–96. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
