

Mechanical and heat hyperalgesia highly predict clinical pain intensity in patients with chronic musculoskeletal pain syndromes
- PMID: 22739051
- PMCID: PMC3581857
- DOI: 10.1016/j.jpain.2012.04.006
Mechanical and heat hyperalgesia highly predict clinical pain intensity in patients with chronic musculoskeletal pain syndromes
Abstract
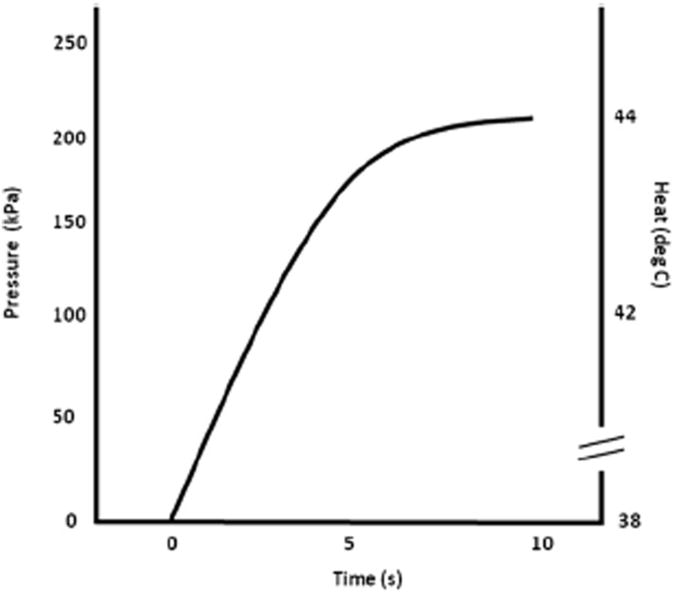
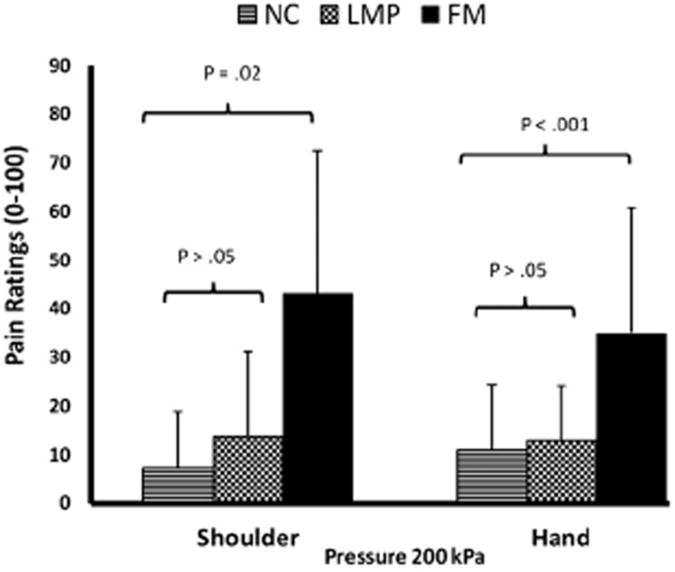
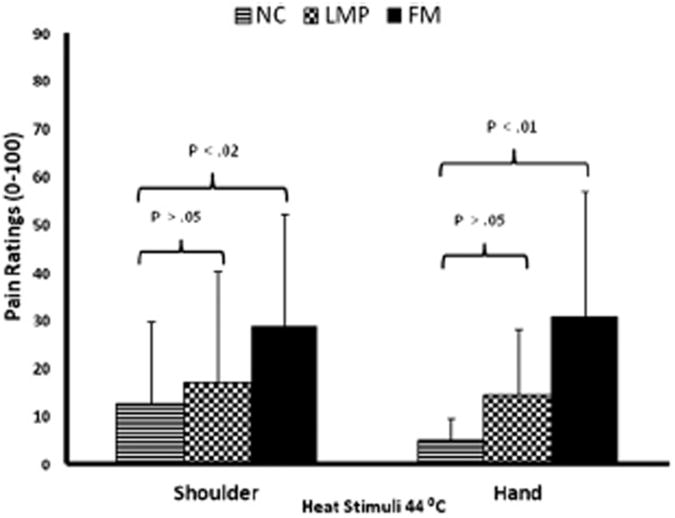
Multiple abnormalities in pain processing have been reported in patients with chronic musculoskeletal pain syndromes. These changes include mechanical and thermal hyperalgesia, decreased thresholds to mechanical and thermal stimuli (allodynia), and central sensitization, all of which are fundamental to the generation of clinical pain. Therefore, we hypothesized that quantitative sensory tests may provide useful predictors of clinical pain intensity of such patients. Our previous studies of fibromyalgia (FM) patients have shown statistically significant correlations of quantitative sensory test results with clinical pain intensity, including mechanical spatial summation, number of pain areas, wind-up, and wind-up aftersensations. Although these tests predicted up to 59% of the variance in FM clinical pain intensity, their expense and technical complexities limited widespread use in clinical practice and trials. Thus, we developed practical tests of primary (mechanical) and secondary (heat) hyperalgesia that also strongly predict clinical pain intensity in patients with chronic musculoskeletal pain disorders. Thirty-six individuals with FM, 24 with local musculoskeletal pain, and 23 normal controls underwent testing of mechanical and heat hyperalgesia at the shoulders and hands. All subjects rated experimental pains using an electronic visual analog scale. Using either heat or pressure pain ratings as well as tender point counts and negative affect as predictors, up to 49.4% of the patients' variance of clinical pain intensity could be estimated. Results of this study emphasize the important contributions of peripheral and central factors to both local and widespread chronic pain. Overall, measures of mechanical and heat hyperalgesia in combination with tender point and negative affect provided powerful predictors of clinical pain intensity in chronic musculoskeletal pain patients that can be readily used in clinical practice and trials.
Perspective: Simple tests of mechanical and heat hyperalgesia can predict large proportions of the variance in clinical pain intensity of chronic musculoskeletal pain patients and thus are feasible to be included in clinical practice and clinical trials.
Copyright © 2012 American Pain Society. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Almay BG. Clinical characteristics of patients with idiopathic pain syndromes. Depressive symptomatology and patient pain drawings. Pain. 1987;29:335–346. - PubMed
-
- Arendt-Nielsen L, Henriksson KG. Pathophysiological mechanisms in chronic musculoskeletal pain (fibromyalgia): The role of central and peripheral sensitization and pain disinhibition. Best Pract Res Clin Rheumatol. 2007;21:465–480. - PubMed
-
- Arroyo JF, Cohen ML. Abnormal responses to electrocutaneous stimulation in fibromyalgia. J Rheumatol. 1993;20:1925–1931. - PubMed
-
- Banic B, Petersen-Felix S, Andersen OK, Radanov BP, Villiger PM, Arendt-Nielsen L, Curatolo M. Evidence for spinal cord hypersensitivity in chronic pain after whiplash injury and in fibromyalgia. Pain. 2004;107:7–15. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
