

Time-resolved imaging of contrast kinetics does not improve performance of follow-up MRA of embolized intracranial aneurysms
- PMID: 22739746
- PMCID: PMC3560766
- DOI: 10.12659/msm.883199
Time-resolved imaging of contrast kinetics does not improve performance of follow-up MRA of embolized intracranial aneurysms
Abstract
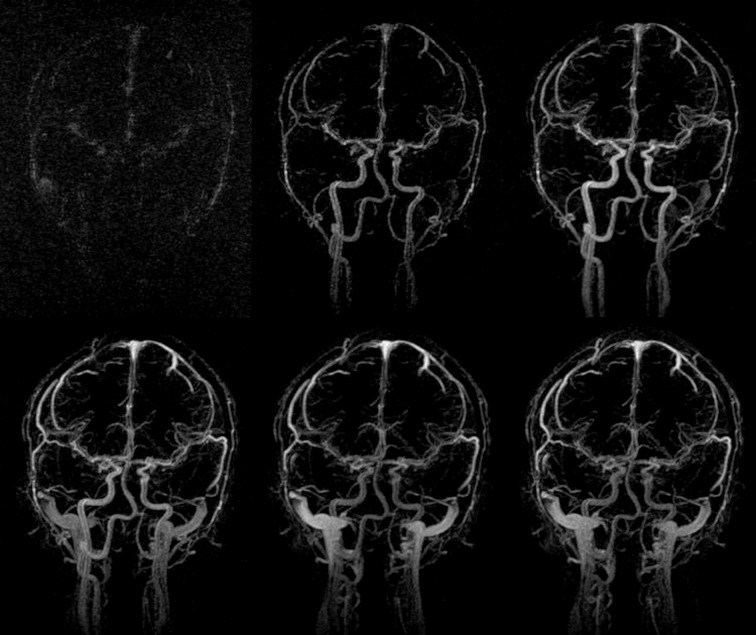
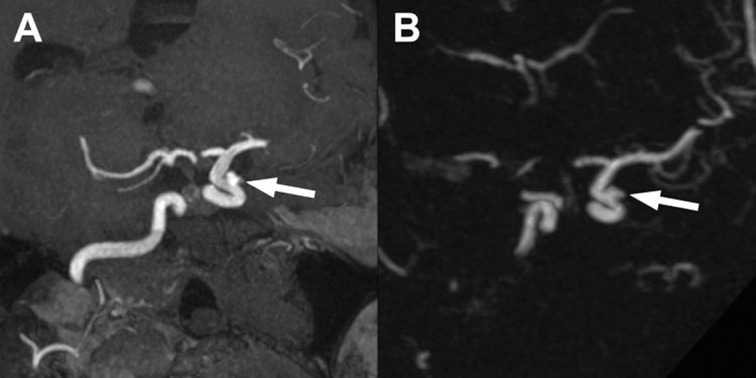
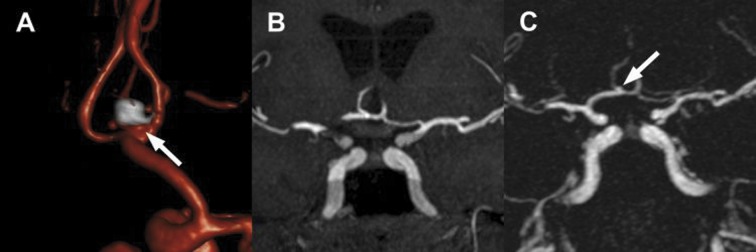
Background: The use of contrast media and the time-resolved imaging of contrast kinetics (TRICKS) technique have some theoretical advantages over time-of-flight magnetic resonance angiography (TOF-MRA) in the follow-up of intracranial aneurysms after endovascular treatment. We prospectively compared the diagnostic performance of TRICKS and TOF-MRA with digital subtracted angiography (DSA) in the assessment of occlusion of embolized aneurysms.
Material/methods: Seventy-two consecutive patients with 72 aneurysms were examined 3 months after embolization. Test characteristics of TOF-MRA and TRICKS were calculated for the detection of residual flow. The results of quantification of flow were compared with weighted kappa. Intraobserver and interobserver reproducibility was determined.
Results: The sensitivity of TOF-MRA was 85% (95% CI, 65-96%) and of TRICKS, 89% (95% CI, 70-97%). The specificity of both methods was 91% (95% CI, 79-98%). The accuracy of the flow quantification ranged from 0.76 (TOF-MRA) to 0.83 (TRICKS). There was no significant difference between the methods in the area under the ROC curve regarding both the detection and the quantification of flow. Intraobserver reproducibility was very good with both techniques (kappa, 0.86-0.89). The interobserver reproducibility was moderate for TOF-MRA and very good for TRICKS (kappa, 0.74-0.80).
Conclusions: In this study, TOF-MRA and TRICKS presented similar diagnostic performance; therefore, the use of time-resolved contrast-enhanced MRA is not justified in the follow-up of embolized aneurysms.
Figures
Similar articles
-
Follow-up after embolization of ruptured intracranial aneurysms: a prospective comparison of two-dimensional digital subtraction angiography, three-dimensional digital subtraction angiography, and time-of-flight magnetic resonance angiography.Neuroradiology. 2012 Nov;54(11):1253-60. doi: 10.1007/s00234-012-1030-z. Epub 2012 Apr 10. Neuroradiology. 2012. PMID: 22488210 Free PMC article.
-
Three-dimensional time-of-flight (3D TOF) magnetic resonance angiography (MRA) and contrast-enhanced MRA of intracranial aneurysms treated with platinum coils.Acta Radiol. 2008 Mar;49(2):190-6. doi: 10.1080/02841850701732940. Acta Radiol. 2008. PMID: 18300146 Clinical Trial.
-
Contrast-Enhanced and Time-of-Flight MRA at 3T Compared with DSA for the Follow-Up of Intracranial Aneurysms Treated with the WEB Device.AJNR Am J Neuroradiol. 2016 Sep;37(9):1684-9. doi: 10.3174/ajnr.A4791. Epub 2016 Apr 21. AJNR Am J Neuroradiol. 2016. PMID: 27102311 Free PMC article.
-
MRA versus DSA for the follow-up imaging of intracranial aneurysms treated using endovascular techniques: a meta-analysis.J Neurointerv Surg. 2019 Oct;11(10):1009-1014. doi: 10.1136/neurintsurg-2019-014936. Epub 2019 May 2. J Neurointerv Surg. 2019. PMID: 31048457 Review.
-
Maximizing time-resolved MRA for differentiation of hemangiomas, vascular malformations and vascularized tumors.Pediatr Radiol. 2012 Jul;42(7):775-84. doi: 10.1007/s00247-012-2359-5. Epub 2012 Mar 8. Pediatr Radiol. 2012. PMID: 22398688 Review.
Cited by
-
Contemporary imaging methods for the follow-up after endovascular abdominal aneurysm repair: a review.Wideochir Inne Tech Maloinwazyjne. 2019 Jan;14(1):1-11. doi: 10.5114/wiitm.2018.78973. Epub 2018 Oct 15. Wideochir Inne Tech Maloinwazyjne. 2019. PMID: 30766622 Free PMC article. Review.
-
Superselective renal artery embolization in the treatment of iatrogenic bleeding into the urinary tract.Med Sci Monit. 2015 Jan 28;21:333-7. doi: 10.12659/MSM.892112. Med Sci Monit. 2015. PMID: 25627580 Free PMC article.
References
-
- Qureshi AI, Vazquez G, Tariq N, et al. Impact of International Subarachnoid Aneurysm Trial results on treatment of ruptured intracranial aneurysms in the United States. J Neurosurg. 2010;114:834–41. - PubMed
-
- Gnanalingham KK, Apostolopoulos V, Barazi S, O’Neill K. The impact of the international subarachnoid aneurysm trial (ISAT) on the management of aneurysmal subarachnoid haemorrhage in a neurosurgical unit in the UK. Clin Neurol Neurosurg. 2006;108:117–23. - PubMed
-
- Ferns SP, Sprengers ME, van Rooij WJ, et al. Coiling of intracranial aneurysms: a systematic review on initial occlusion and reopening and retreatment rates. Stroke. 2009;40:e523–29. - PubMed
-
- Ringer AJ, Rodriguez-Mercado R, Veznedaroglu E, et al. Defining the risk of retreatment for aneurysm recurrence or residual after initial treatment by endovascular coiling: a multicenter study. Neurosurgery. 2009;65:311–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
