

Hypoplastic right-heart syndrome presenting as multiple miscarriages
- PMID: 22740745
- PMCID: PMC3384066
Hypoplastic right-heart syndrome presenting as multiple miscarriages
Abstract
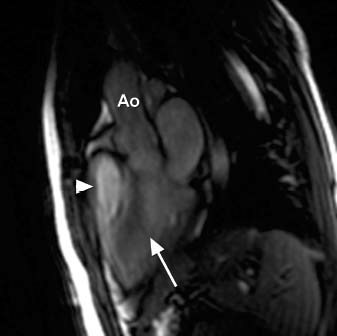
Reversible causes of miscarriage are many, but they affect only 1% of women who are trying to conceive. Herein, we describe the case of a 23-year-old woman who presented for evaluation of repeated miscarriages and was found to have hypoxemia and erythrocytosis. Further evaluation revealed hypoplastic right-heart syndrome with an intracardiac shunt. She underwent hybrid repair with pulmonary valve balloon valvuloplasty, followed by surgery to perform atrial septal defect closure and a Glenn anastomosis. The erythrocytosis and hypoxemia resolved, and she was able to conceive and deliver a healthy baby at term 2 years later. This is a unique case of a rare congenital heart defect that went unnoticed until adulthood, when attempts at pregnancy failed because of the associated hypoxemia. Timely and appropriate treatment led to a successful pregnancy after repeated miscarriages. This case exemplifies the need for a comprehensive medical evaluation of every woman with a history of multiple miscarriages to determine whether a reversible cause exists.
Keywords: Abortion, spontaneous/etiology; heart defects, congenital/complications/physiopathology/therapy/surgery; treatment outcome; ventricular function, right/physiology.
Figures








References
-
- Tzioras S, Polyzos NP, Economides DL. How do you solve the problem of recurrent miscarriage? Reprod Biomed Online 2009;19(3):296–7. - PubMed
-
- Griesshammer M, Struve S, Harrison CM. Essential thrombocythemia/polycythemia vera and pregnancy: the need for an observational study in Europe. Semin Thromb Hemost 2006;32(4 Pt 2):422–9. - PubMed
-
- Brickner ME, Hillis LD, Lange RA. Congenital heart disease in adults. Second of two parts [published erratum appears in N Engl J Med 2000;342(13):988]. N Engl J Med 2000; 342(5):334–42. - PubMed
-
- Prasad K, Singh M, Radhakrishnan S. Hypoplastic right ventricle with mild pulmonary stenosis in an adult. Int J Cardiol 1992;37(2):260–2. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources