

Risk factors for postoperative respiratory complications following esophageal cancer resection
- PMID: 22741016
- PMCID: PMC3362471
- DOI: 10.3892/ol.2012.589
Risk factors for postoperative respiratory complications following esophageal cancer resection
Abstract
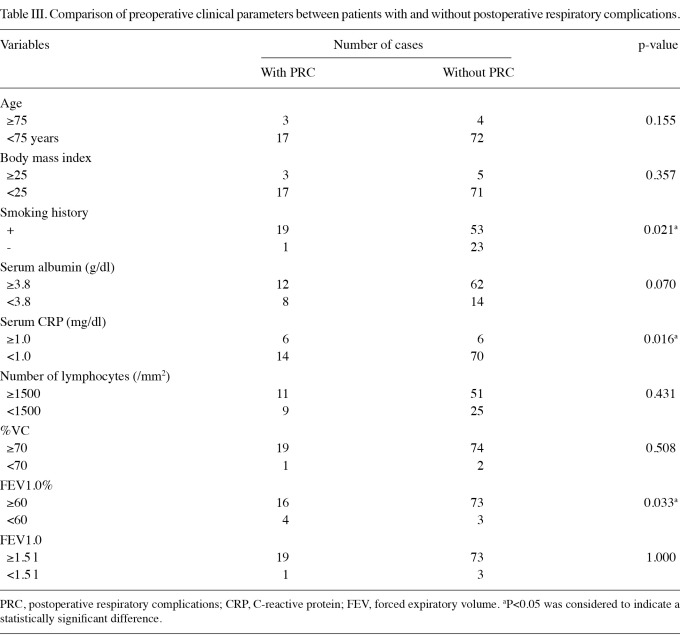
The development of surgical and postoperative management techniques has improved the treatment outcomes of esophageal cancer resection. However, respiratory morbidity is still the most frequent complication after esophagectomy. The objective of the present study was to identify risk factors for respiratory complications following resection for esophageal cancer. This study included 96 patients with esophageal cancer who had undergone esophagectomy with lymph node dissection. The patients were divided into 2 groups according to the presence (20 patients, 17 had pneumonia and 3 had acute respiratory distress syndrome) or absence (76 patients) of postoperative respiratory complications (PRC). The two groups were compared with respect to their preoperative clinical variables, such as age, body mass index, smoking history, serum albumin, serum C-reactive protein (CRP), number of lymphocytes, %VC, FEV1.0% and FEV1.0. Furthermore, multiple logistic regression analyses were used to estimate relative risk factors for respiratory complications. Results of the univariate analysis showed that smoking history (+/-, patients with PRC, 19/1 and without PRC, 53/23), serum CRP (≥1.0 mg/dl/<1.0 mg/dl, patients with PRC, 6/14 and without PRC, 6/70) and FEV1.0% (≥60%/<60%, patients with PRC, 16/4 and without PRC, 73/3) were significantly different between the two groups. Multiple logistic regression analysis showed that FEV1.0% was the strongest predictor of PRC. FEV1.0%, serum CRP and smoking history are reliable predictors of the risk of respiratory complications following esophageal cancer resection. For patients with these factors, perioperative management for the prevention of postoperative respiratory complications should be considered.
Figures




References
-
- Tachibana M, Kinugasa S, Yoshimura H, Shibakita M, Tonomoto Y, Dhar DK, Nagasue N. Clinical outcomes of extended esophagectomy with three-field lymph node dissection for esophageal squamous cell carcinoma. Am J Surg. 2005;189:98–109. - PubMed
-
- Ferguson MK, Durkin AE. Preoperative prediction of the risk of pulmonary complications after esophagectomy for cancer. J Thorac Cardiovasc Surg. 2002;123:661–669. - PubMed
-
- Bailey SH, Bull DA, Harpole DH, Rentz JJ, Neumayer LA, Pappas TN, Daley J, Henderson WG, Krasnicka B, Khuri SF. Outcomes after esophagectomy: a ten-year prospective cohort. Ann Thorac Surg. 2003;75:217–222. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous